

Does Humeral Component Lateralization in Reverse Shoulder Arthroplasty Affect Rotator Cuff Torque? Evaluation in a Cadaver Model
- PMID: 28616758
- PMCID: PMC5599403
- DOI: 10.1007/s11999-017-5413-7
Does Humeral Component Lateralization in Reverse Shoulder Arthroplasty Affect Rotator Cuff Torque? Evaluation in a Cadaver Model
Abstract
Background: Humeral component lateralization in reverse total shoulder arthroplasty (RTSA) may improve the biomechanical advantage of the rotator cuff, which could improve the torque generated by the rotator cuff and increase internal and external rotation of the shoulder.
Purpose: The purpose of this in vitro biomechanical study was to evaluate the effect of humeral component lateralization (or lateral offset) on the torque of the anterior and posterior rotator cuff.
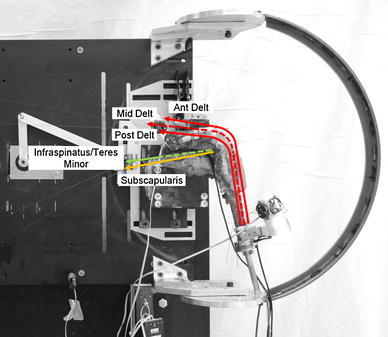
Methods: Eight fresh-frozen cadaveric shoulders from eight separate donors (74 ± 8 years; six males, two females) were tested using an in vitro simulator. All shoulders were prescreened for soft tissue deficit and/or deformity before testing. A custom RTSA prosthesis was implanted that allowed five levels of humeral component lateralization (15, 20, 25, 30, 35 mm), which avoided restrictions imposed by commercially available designs. The torques exerted by the anterior and posterior rotator cuff were measured three times and then averaged for varying humeral lateralization, abduction angle (0°, 45°, 90°), and internal and external rotation (-60°, -30°, 0°, 30°, 60°). A three-way repeated measures ANOVA (abduction angle, humeral lateralization, internal rotation and external rotation angles) with a significance level of α = 0.05 was used for statistical analysis.
Results: Humeral lateralization only affected posterior rotator cuff torque at 0° abduction, where increasing humeral lateralization from 15 to 35 mm at 60° internal rotation decreased external rotation torque by 1.6 ± 0.4 Nm (95% CI, -0.07 -1.56 Nm; p = 0.06) from 4.0 ± 0.3 Nm to 2.4 ± 0.6 Nm, respectively, but at 60° external rotation increased external rotation torque by 2.2 ± 0.5 Nm (95% CI, -4.2 to -0.2 Nm; p = 0.029) from 6.2 ± 0.5 Nm to 8.3 ± 0.5 Nm, respectively. Anterior cuff torque was affected by humeral lateralization in more arm positions than the posterior cuff, where increasing humeral lateralization from 15 to 35 mm when at 60° internal rotation increased internal rotation torque at 0°, 45°, and 90° abduction by 3.2 ± 0.5 Nm (95% CI, 1.1-5.2 Nm; p = 0.004) from 6.6 ± 0.6 Nm to 9.7 ± 0.6 Nm, 4.0 ± 0.3 Nm (95% CI, 2.8-5.0 Nm; p < 0.001) from 1.7 ± 1.0 Nm to 5.6 ± 0.9 Nm, and 2.2 ± 0.2 Nm (95% CI, 1.4-2.9 Nm; p < 0.001) from 0.6 ± 0.6 Nm to 2.8 ± 0.6 Nm, respectively. In neutral internal and external rotation, increasing humeral lateral offset from 15 to 35 mm increased the internal rotation torque at 45˚ and 90˚ abduction by 1.5 ± 0.3 Nm (95% CI, 0.2-2.7 Nm; p = 0.02) and 1.3 ± 0.2 Nm (95% CI, 0.4-2.3 Nm; p < 0.001), respectively.
Conclusions: Humeral component lateralization improves rotator cuff torque.
Clinical relevance: The results of this preliminary in vitro cadaveric study suggest that the lateral offset of the RTSA humeral component plays an important role in the torque generated by the anterior and posterior rotator cuff. However, further studies are needed before clinical application of these results. Increasing humeral offset may have adverse effects, such as the increased risk of implant modularity, increasing tension of the cuff and soft tissues, increased costs often associated with design modifications, and other possible as yet unforeseen negative consequences.
Figures




Comment in
-
CORR Insights®: Does Humeral Component Lateralization in Reverse Shoulder Arthroplasty Affect Rotator Cuff Torque? Evaluation in a Cadaver Model.Clin Orthop Relat Res. 2017 Oct;475(10):2572-2574. doi: 10.1007/s11999-017-5460-0. Epub 2017 Aug 7. Clin Orthop Relat Res. 2017. PMID: 28786089 Free PMC article. No abstract available.
References
-
- Affonso J, Nicholson GP, Frankle MA, Walch G, Gerber C, Garzon-Muvdi J, McFarland EG. Complications of the reverse prosthesis: prevention and treatment. Instr Course Lect. 2012;61:157–168. - PubMed
-
- Alta TD, Veeger DH, de Toledo JM, Janssen TW, Willems WJ. Isokinetic strength differences between patients with primary reverse and total shoulder prostheses: muscle strength quantified with a dynamometer. Clin Biomech (Bristol, Avon). 2014;29:965–970. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
