

Medical Therapy and Recurrent Ischemic Events in High Risk Patients Surviving their Myocardial Infarction for at Least 12 Months: Comparison of Patients with ST Elevation Versus Non-ST Elevation Myocardial Infarction
- PMID: 28616861
- PMCID: PMC5688970
- DOI: 10.1007/s40119-017-0093-7
Medical Therapy and Recurrent Ischemic Events in High Risk Patients Surviving their Myocardial Infarction for at Least 12 Months: Comparison of Patients with ST Elevation Versus Non-ST Elevation Myocardial Infarction
Abstract
Introduction: Data about treatments and recurrent ischemic events in patients surviving their most recent myocardial infarction event-free for at least 12 months are scarce.
Methods: In a retrospective data analysis, charts of patients who had a myocardial infarction 1-3 years ago with an event-free period of at least 12 months after the index event and at least one high risk factor were centrally collected and analyzed. Here we compare patients with ST elevation myocardial infarction (STEMI) versus non-ST elevation myocardial infarction (NSTEMI).
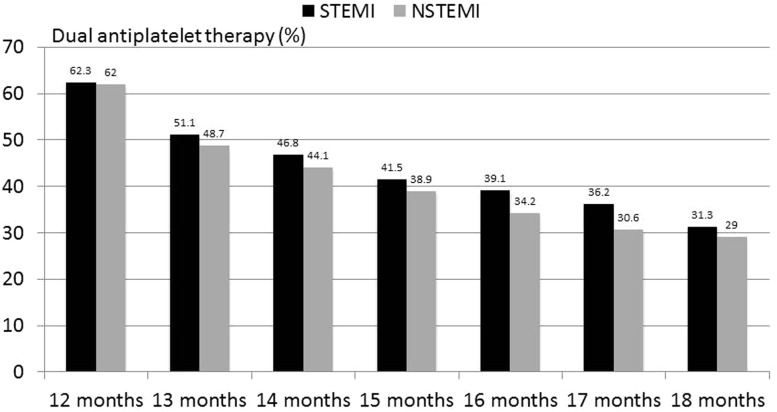
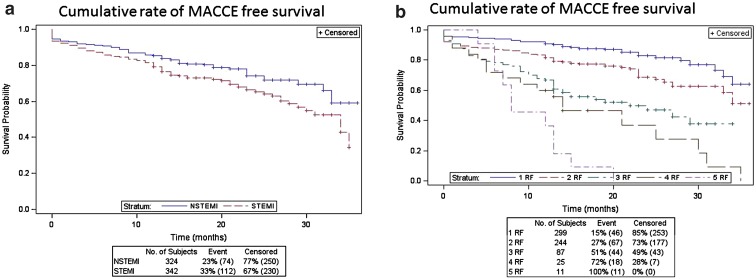
Results: A total of 666 patients, 342 with STEMI and 324 with NSTEMI, were included. Revascularization procedures for the index event were performed in 89% of patients with STEMI and 72% of patients with NSTEMI. About 62% of patients were still on dual antiplatelet therapy after 12 months, predominantly with aspirin and clopidogrel. This rate declined to 30% after 18 months. Patients with STEMI had a higher mortality (19% versus 13%, p = 0.04) and major adverse cardiovascular and cerebrovascular event rate (MACCE; 33% versus 23%, p = 0.03) during follow-up up to 36 months, while there were no significant differences with respect to recurrent myocardial infarction or stroke. The number of high risk factors was closely linked to the rate of MACCE at follow up.
Conclusions: Patients surviving their myocardial infarction without any further event during the first 12 months have a high rate of recurrent ischemic events in both STEMI and NSTEMI cases during subsequent follow-up. Therefore, secondary prevention therapies should be continued even one year after myocardial infarction, which might improve outcomes.
Keywords: Acute myocardial infarction; Prognosis; Secondary prevention.
Figures
References
-
- Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:267–315. doi: 10.1093/eurheartj/ehv320. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
