

Longitudinal Patterns of Medication Nonadherence and Associated Health Care Costs
- PMID: 28617754
- PMCID: PMC5561465
- DOI: 10.1097/MIB.0000000000001165
Longitudinal Patterns of Medication Nonadherence and Associated Health Care Costs
Abstract
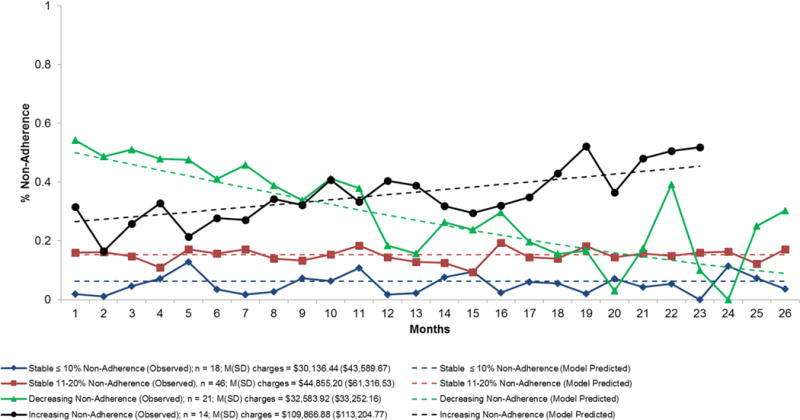
Background: Nonadherence to treatment recommendations is associated with poorer outcomes in inflammatory bowel disease and may increase the cost of care. We examined the longitudinal relationship between nonadherence and health care costs and hypothesized that at least 3 distinct trajectories of nonadherence would be observed and that increasing nonadherence would account for significantly greater health care costs after controlling for disease activity.
Methods: Ninety-nine patients aged 2 to 21 years with inflammatory bowel disease were recruited into this 2-year longitudinal study. Medication possession ratios were calculated from pharmacy refill data, disease activity ratings were obtained from medical charts, and hospital and physician charges associated with an International Classification of Diseases, Ninth Revision code for ulcerative colitis or Crohn's disease were obtained from the hospital's accounting database.
Results: An average total cost effect size of d = 0.68 was observed between the increasing severity and stable low severity groups, but the confidence intervals overlap. Conversely, patients with increasing nonadherence demonstrated significantly higher health care costs than patients with stable ≤10%, stable 11% to 20%, or decreasing nonadherence.
Conclusions: Medication nonadherence is related to increased health care costs after controlling for disease severity. Patients with increasing nonadherence over time demonstrate more than a 3-fold increase in costs compared with adherent patients. In addition, patients whose adherence improves over time incur approximately the same costs as those who are consistently adherent. This suggests that, in addition to leveraging prevention efforts to keep patients from becoming more nonadherent as treatment continues, efforts aimed at modifying adherence behavior may result in significant cost savings over time.
Figures
References
-
- Services CfMaM. NHE Summary including share of GDP, CY 1960–2013. 2014
-
- Martin AB, Lassman D, Washington B, Catlin A, Team NHEA Growth In US Health Spending Remained Slow In 2010; Health Share Of Gross Domestic Product Was Unchanged From 2009. Health Affairs. 2012;31(1):208–219. - PubMed
-
- Davis K, Stremikis K, Schoen C, Squires D. Mirror, Mirror on the Wall, 2014 Update: How the U.S. Health Care System Compares Internationally. Vol June 2014. The Commonwealth Fund. 2014
-
- Burwell SM. Setting Value-Based Payment Goals — HHS Efforts to Improve U.S. Health Care. New England Journal of Medicine. 2015;372(10):897–899. - PubMed
-
- Better, Smarter, Healthier: In historic announcement, HHS sets clear goals and timeline for shifting Medicare reimbursements from volume to value [press release] 2015 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
