

Cost-effectiveness of HPV-based cervical cancer screening in the public health system in Nicaragua
- PMID: 28619772
- PMCID: PMC5623348
- DOI: 10.1136/bmjopen-2016-015048
Cost-effectiveness of HPV-based cervical cancer screening in the public health system in Nicaragua
Abstract
Objectives: To evaluate the cost-effectiveness of human papillomavirus (HPV) DNA testing (versus Papanicolaou (Pap)-based screening) for cervical cancer screening in Nicaragua.
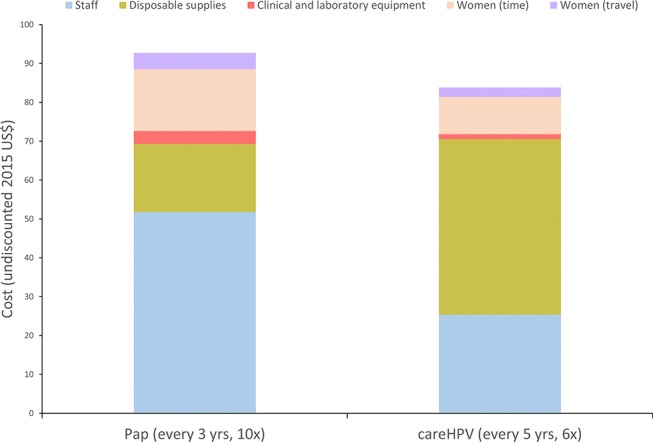
Design: A previously developed Monte Carlo simulation model of the natural history of HPV infection and cervical cancer was calibrated to epidemiological data from Nicaragua. Cost data inputs were derived using a micro-costing approach in Carazo, Chontales and Chinandega departments; test performance data were from a demonstration project in Masaya department.
Setting: Nicaragua's public health sector facilities.
Participants: Women aged 30-59 years.
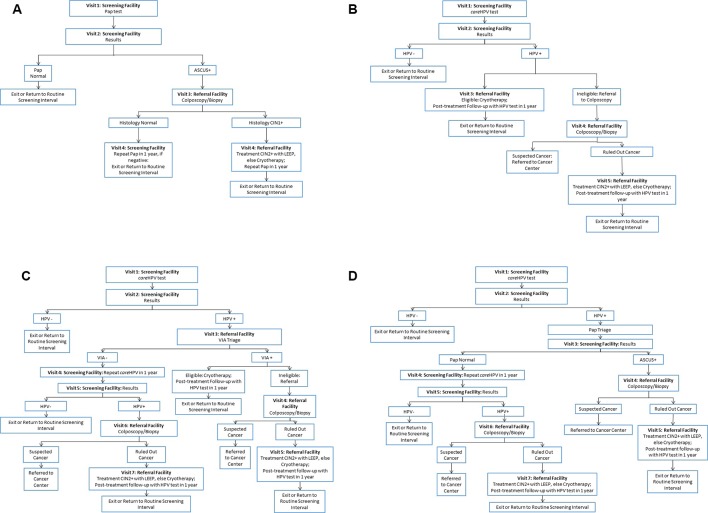
Interventions: Screening strategies included (1) Pap testing every 3 years, with referral to colposcopy for women with an atypical squamous cells of undetermined significance or worse result ('Pap'); (2) HPV testing every 5 years, with referral to cryotherapy for HPV-positive eligible women (HPV cryotherapy or 'HPV-Cryo'); (3) HPV testing every 5 years, with referral to triage with visual inspection with acetic acid (VIA) for HPV-positive women ('HPV-VIA'); and (4) HPV testing every 5 years, with referral to Pap testing for HPV-positive women ('HPV-Pap').
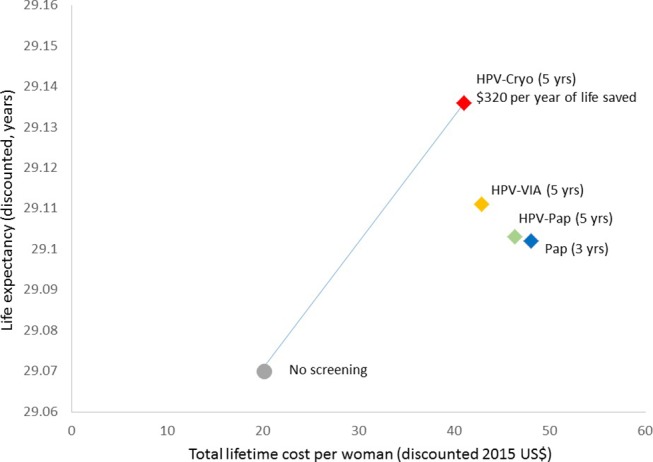
Outcome measures: Reduction in lifetime risk of cancer and incremental cost-effectiveness ratios (ICER; 2015 US$ per year of life saved (YLS)).
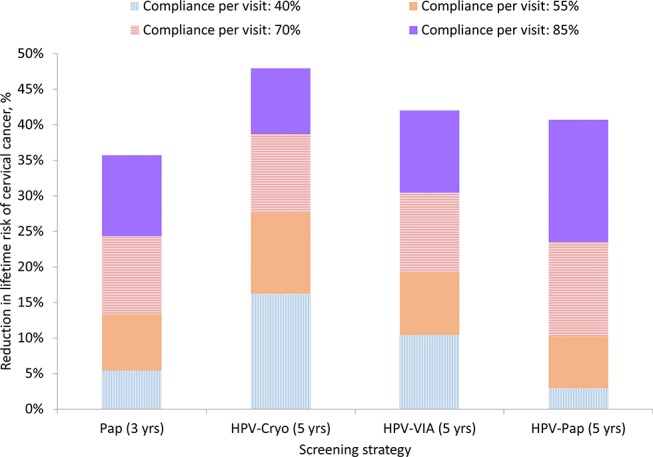
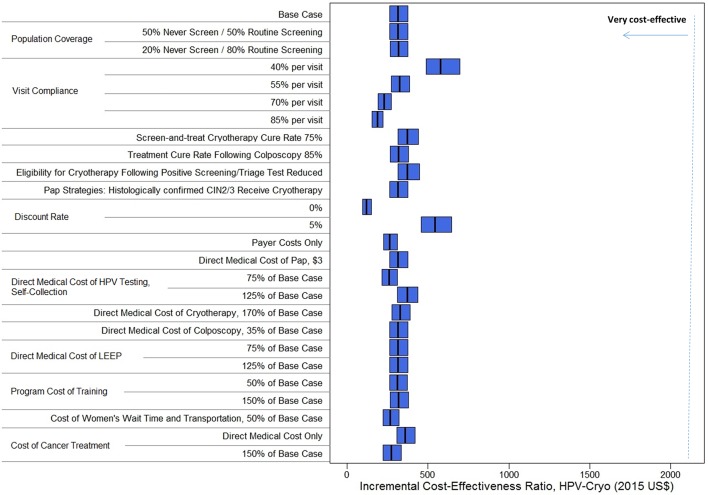
Results: HPV-based screening strategies were more effective than Pap testing. HPV-Cryo was the least costly and most effective strategy, reducing lifetime cancer risk by 29.5% and outperforming HPV-VIA, HPV-Pap and Pap only, which reduced cancer risk by 19.4%, 12.2% and 10.8%, respectively. With an ICER of US$320/YLS, HPV-Cryo every 5 years would be very cost-effective using a threshold based on Nicaragua's per capita gross domestic product of US$2090. Findings were robust across sensitivity analyses on test performance, coverage, compliance and cost parameters.
Conclusions: HPV testing is very cost-effective compared with Pap testing in Nicaragua, due to higher test sensitivity and the relatively lower number of visits required. Increasing compliance with recommended follow-up will further improve the health benefits and value for public health dollars.
Keywords: epidemiology; health economics; public health.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JJ was the director of the START-UP demonstration projects and received all tests used in the study as a donation from Qiagen; no other relationships or activities that could appear to have influenced the submitted work. JJ was the co-owner and Deputy Manager of Onco Prev International, a Peruvian company, from 2012 through March 2017. Onco Prev International offers cervical cancer screening services and in 2016 also began positioning for distribution of medical devices including colposcopes and the Liger thermocoagulator. Onco Prev International did not commercialize any medical instrument during the time JJ was part of the company.
Figures
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer, 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials