

Mitochondrial Integrity and Function in the Progression of Early Pressure Overload-Induced Left Ventricular Remodeling
- PMID: 28619984
- PMCID: PMC5669187
- DOI: 10.1161/JAHA.117.005869
Mitochondrial Integrity and Function in the Progression of Early Pressure Overload-Induced Left Ventricular Remodeling
Abstract
Background: Following pressure overload, compensatory concentric left ventricular remodeling (CR) variably transitions to eccentric remodeling (ER) and systolic dysfunction. Mechanisms responsible for this transition are incompletely understood. Here we leverage phenotypic variability in pressure overload-induced cardiac remodeling to test the hypothesis that altered mitochondrial homeostasis and calcium handling occur early in the transition from CR to ER, before overt systolic dysfunction.
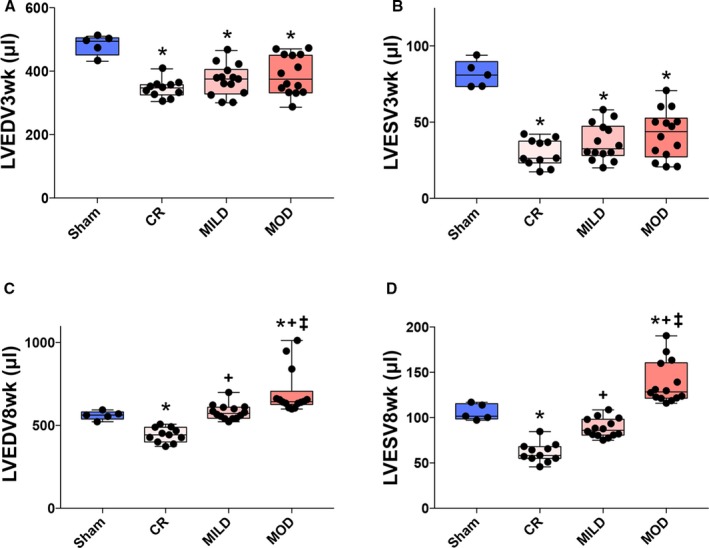
Methods and results: Sprague Dawley rats were subjected to ascending aortic banding, (n=68) or sham procedure (n=5). At 3 weeks post-ascending aortic banding, all rats showed CR (left ventricular volumes < sham). At 8 weeks post-ascending aortic banding, ejection fraction was increased or preserved but 3 geometric phenotypes were evident despite similar pressure overload severity: persistent CR, mild ER, and moderate ER with left ventricular volumes lower than, similar to, and higher than sham, respectively. Relative to sham, CR and mild ER phenotypes displayed increased phospholamban, S16 phosphorylation, reduced sodium-calcium exchanger expression, and increased mitochondrial biogenesis/content and normal oxidative capacity, whereas moderate ER phenotype displayed decreased p-phospholamban, S16, increased sodium-calcium exchanger expression, similar degree of mitochondrial biogenesis/content, and impaired oxidative capacity with unique activation of mitochondrial autophagy and apoptosis markers (BNIP3 and Bax/Bcl-2).
Conclusions: After pressure overload, mitochondrial biogenesis and function and calcium handling are enhanced in compensatory CR. The transition to mild ER is associated with decrease in mitochondrial biogenesis and content; however, the progression to moderate ER is associated with enhanced mitochondrial autophagy/apoptosis and impaired mitochondrial function and calcium handling, which precede the onset of overt systolic dysfunction.
Keywords: heart failure; hypertrophy; mitochondria; remodeling.
© 2017 The Authors and Mayo Clinic. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures







References
-
- McMurray JJ, Petrie MC, Murdoch DR, Davie AP. Clinical epidemiology of heart failure: public and private health burden. Eur Heart J. 1998;19(Suppl P):P9–P16. - PubMed
-
- Nichols M, Townsend N, Scarborough P, Rayner M. Cardiovascular disease in Europe 2014: epidemiological update. Eur Heart J. 2014;35:2950–2959. - PubMed
-
- Williamson JD, Supiano MA, Applegate WB, Berlowitz DR, Campbell RC, Chertow GM, Fine LJ, Haley WE, Hawfield AT, Ix JH, Kitzman DW, Kostis JB, Krousel‐Wood MA, Launer LJ, Oparil S, Rodriguez CJ, Roumie CL, Shorr RI, Sink KM, Wadley VG, Whelton PK, Whittle J, Woolard NF, Wright JT Jr, Pajewski NM. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. JAMA. 2016;315:2673–2682. - PMC - PubMed
-
- Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure‐lowering treatment. 6. Prevention of heart failure and new‐onset heart failure–meta‐analyses of randomized trials. J Hypertens 2016;34:373–384; discussion 384. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
