

Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review
- PMID: 28620520
- PMCID: PMC5424401
- DOI: 10.1186/s40738-015-0008-z
Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review
Abstract
Background: Ectopic pregnancy is a potentially life-threatening condition occurring in 1-2 % of all pregnancies. The most common ectopic implantation site is the fallopian tube, though 10 % of ectopic pregnancies implant in the cervix, ovary, myometrium, interstitial portion of the fallopian tube, abdominal cavity or within a cesarean section scar.
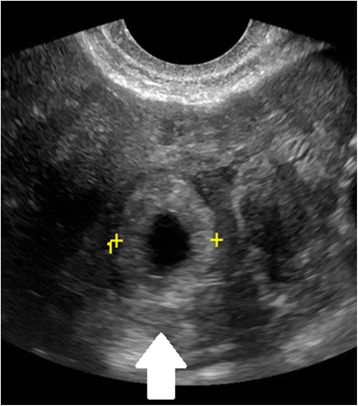
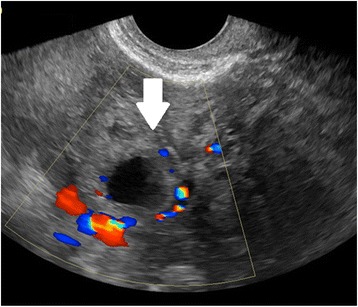
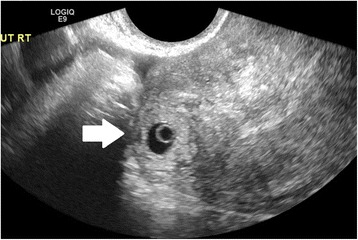
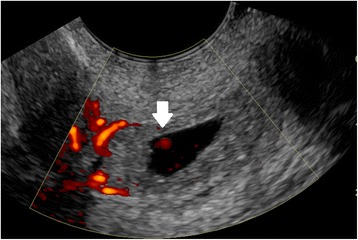
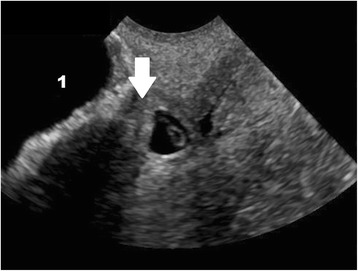
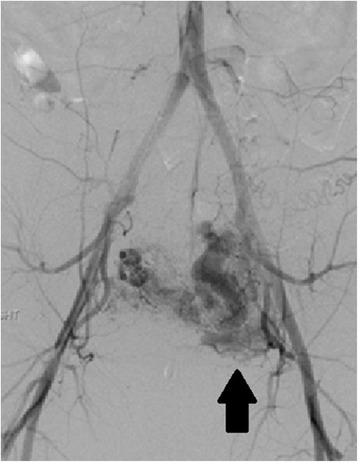
Findings: Diagnosis involves a combination of clinical symptoms, serology, and ultrasound. Medical management is a safe and effective option in most clinically stable patients. Patients who have failed medical management, are ineligible, or present with ruptured ectopic pregnancy or heterotopic pregnancy are most often managed with excision by laparoscopy or, less commonly, laparotomy. Management of nontubal ectopic pregnancies may involve medical or surgical treatment, or a combination, as dictated by ectopic pregnancy location and the patient's clinical stability. Following tubal ectopic pregnancy, the rate of subsequent intrauterine pregnancy is high and independent of treatment modality.
Conclusion: This review describes the incidence, risk factors, diagnosis, and management of tubal and non-tubal ectopic and heterotopic pregnancies, and reviews the existing data regarding recurrence and future fertility.
Keywords: Ectopic pregnancy; Heterotopic pregnancy; Nontubal ectopic pregnancy.
Figures



References
-
- Hoffman BL, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham F, et al. Chapter 7. Ectopic pregnancy. In: Hoffman BL, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham F, Calver LE, et al., editors. Williams gynecology. 2. New York: McGraw-Hill; 2012.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
