

Comparison of uterine and tubal pathology identified by transvaginal sonography, hysterosalpingography, and hysteroscopy in female patients with infertility
- PMID: 28620525
- PMCID: PMC5424419
- DOI: 10.1186/s40738-015-0012-3
Comparison of uterine and tubal pathology identified by transvaginal sonography, hysterosalpingography, and hysteroscopy in female patients with infertility
Abstract
Background: The causes of female infertility are multifactorial and necessitate comprehensive evaluation including physical examination, hormonal testing, and imaging. Given the associated psychological and financial stress that imaging can cause, infertility patients benefit from a structured and streamlined evaluation. The goal of such a work up is to evaluate the uterus, endometrium, and fallopian tubes for anomalies or abnormalities potentially preventing normal conception. To date, the standard method for assessing these structures typically involves some combination of transvaginal sonography (TVS), hysterosalpingography (HSG), and hysteroscopy (HSC). The goal of this review is to compare the diagnostic accuracy of TVS, HSG, and HSC for diagnosing abnormalities in infertility patients to determine if all studies are necessary for pre-treatment evaluation.
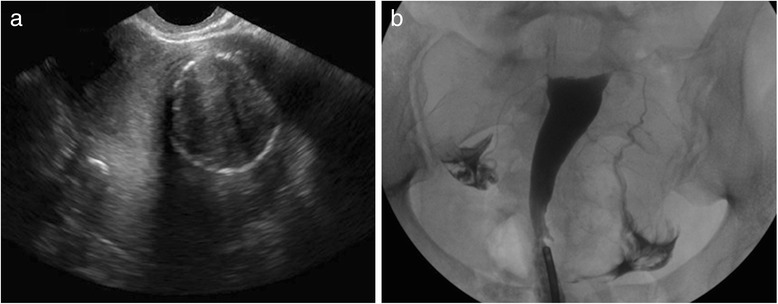
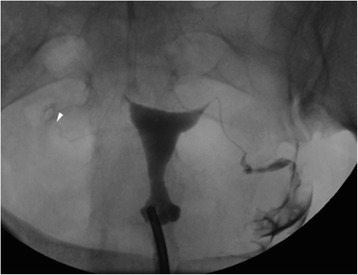
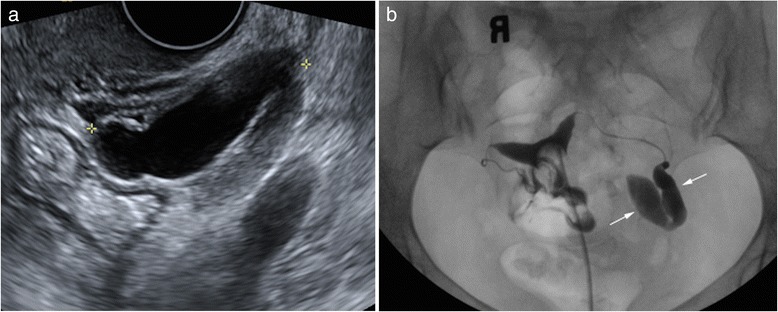
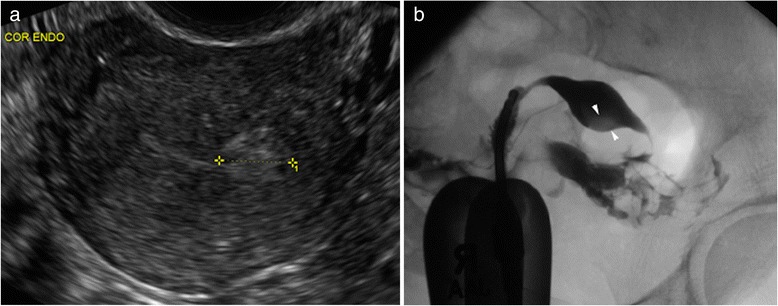
Results: We identified infertility patients prior to initiation of assisted reproductive technology who had baseline TVS, HSG, and HSC within 180 days of each other. From medical record review, we compared frequencies of each finding between modalities. Of the 1274 patients who received a baseline TVS over 2 years, 327 had TVS and HSG within 180 days and 55 patients had TVS, HSG and HSC. Of the 327, TVS detected fibroids more often than HSG (74 vs. 5, p < .0001), and adenomyosis more often than HSG (7 vs. 2, p = .02). HSG detected tubal obstruction more often than TVS (56 vs. 8, p = .002). Four (1.2 %) patients had endometrial polyps on both HSG and TVS. In the 55 patients with HSG, TVS, and HSC, HSC identified endometrial polyps more often than TVS (10 vs. 1, p = .0001) and HSG (10 vs. 2, p = .0007). TVS detected more fibroids than HSC (17 vs. 5, p < .0001). Tubal obstruction was identified more often by HSG than HSC (19 vs. 5, p < .0001).
Conclusions: TVS is superior for evaluation of myometrial pathology. HSG is superior for evaluation of tubal pathologies. Endometrial pathologies are best identified with HSC.
Keywords: Hysterosalpingography; Infertility; Transvaginal sonography.
Figures
References
-
- Chandra A, Martinez GM, Mosher WD, Abma JC, Jones J. Fertility, family planning, and reproductive health of U.S. women: data from 2002 National Survey of Family Growth. Vital Health Stat. 2012;23:1–160. - PubMed
-
- Chandran A, Copen CE, Stephen EH. Infertility service use in the United States: Data from the National survey of Family Growth, 1982-2010. http://www.cdc.gov/nchs/data/nhsr/nhsr073.pdf - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
