

Tracheobronchomalacia Is Associated with Increased Morbidity in Bronchopulmonary Dysplasia
- PMID: 28622012
- PMCID: PMC5711403
- DOI: 10.1513/AnnalsATS.201702-178OC
Tracheobronchomalacia Is Associated with Increased Morbidity in Bronchopulmonary Dysplasia
Abstract
Rationale: Tracheobronchomalacia is a common comorbidity in neonates with bronchopulmonary dysplasia. However, the effect of tracheobronchomalacia on the clinical course of bronchopulmonary dysplasia is not well-understood.
Objective: We sought to assess the impact of tracheobronchomalacia on outcomes in neonates with bronchopulmonary dysplasia in a large, multi-center cohort.
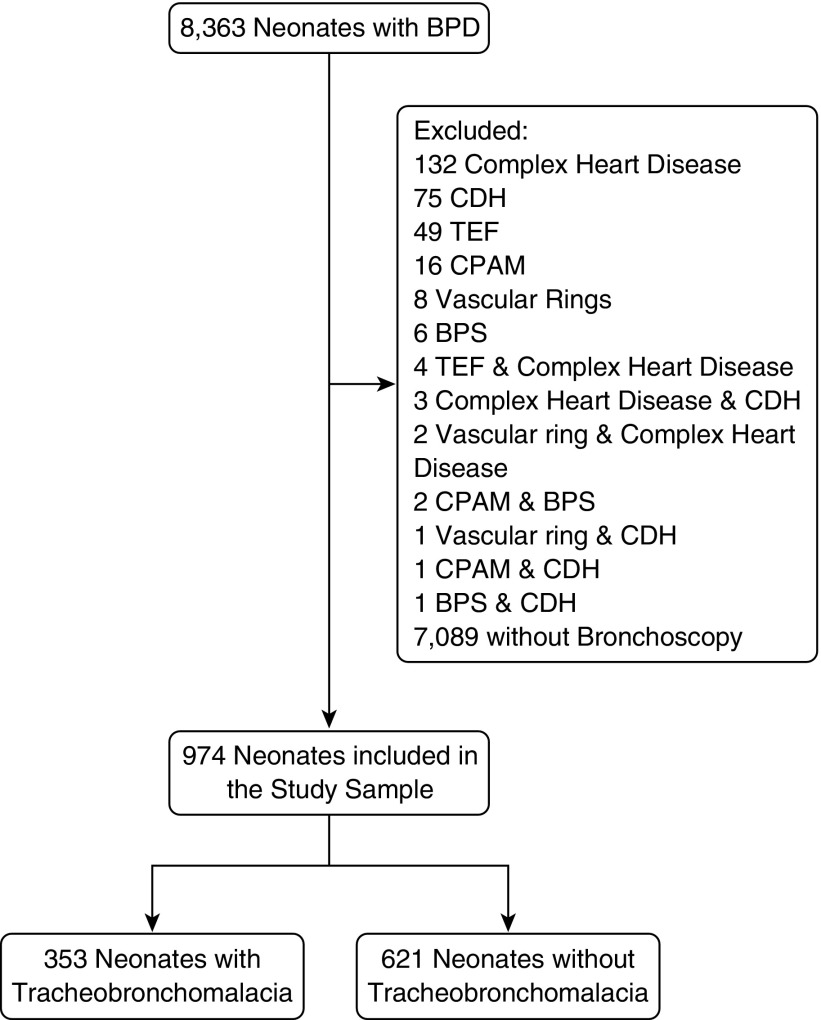
Methods: We preformed a cohort study of 974 neonates with bronchopulmonary dysplasia admitted to 27 neonatal intensive care units participating in the Children's Hospital Neonatal Database who had undergone bronchoscopy. In hospital morbidity for neonates with bronchopulmonary dysplasia and tracheobronchomalacia (N=353, 36.2%) was compared to those without tracheobronchomalacia (N=621, 63.8%) using mixed-effects multivariate regression.
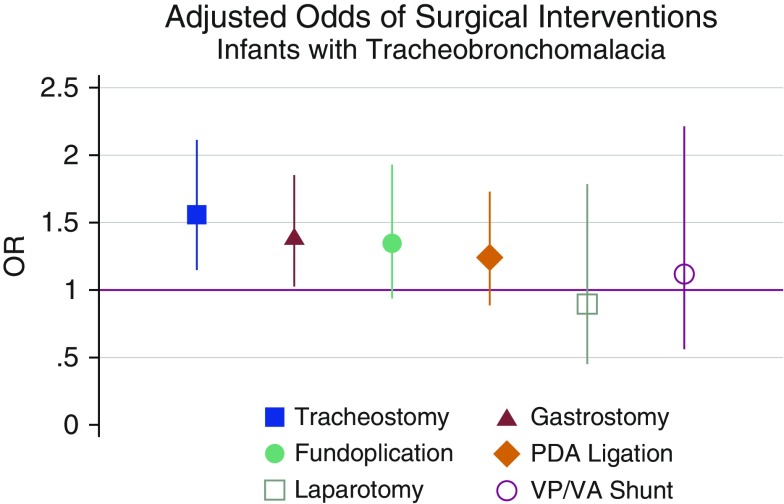
Results: Neonates with tracheobronchomalacia and bronchopulmonary dysplasia had more comorbidities, such as gastroesophageal reflux (OR=1.65, 95%CI 1.23- 2.29, P=0.001) and pneumonia (OR=1.68, 95%CI 1.21-2.33, P=0.002) and more commonly required surgeries such as tracheostomy (OR=1.55, 95%CI 1.15-2.11, P=0.005) and gastrostomy (OR=1.38, 95%CI 1.03-1.85, P=0.03) compared with those without tracheobronchomalacia. Neonates with tracheobronchomalacia were hospitalitized (118 ± 93 vs 105 ± 83 days, P=0.02) and ventilated (83.1 ± 91.1 vs 67.2 ± 71.9 days, P=0.003) longer than those without tracheobronchomalacia. Upon discharge, neonates with tracheobronchomalacia and BPD were more likely to be mechanically ventilated (OR=1.37, 95CI 1.01-1.87 P=0.045) and possibly less likely to receive oral nutrition (OR=0.69, 95%CI 0.47-1.01, P=0.058).
Conclusions: Tracheobronchomalacia is common in neonates with bronchopulmonary dysplasia who undergo bronchoscopy and is associated with longer and more complicated hospitalizations.
Figures

Comment in
-
Tracheobronchomalacia in Neonates: The "New Bronchopulmonary Dysplasia" Is Not Just about the Alveoli.Ann Am Thorac Soc. 2017 Sep;14(9):1387-1388. doi: 10.1513/AnnalsATS.201706-507ED. Ann Am Thorac Soc. 2017. PMID: 28862496 No abstract available.
References
-
- Holinger PH, Johnston KC, Parchet VN, Zimmermann AA. Congenital malformations of the trachea, bronchi and lung. Trans Annu Meet Am Bronchoesophagol Assoc. 1952;58:67–88. - PubMed
-
- Baxter JD, Dunbar JS. Tracheomalacia. Ann Otol Rhinol Laryngol. 1963;72:1013–1023. - PubMed
-
- Mair EA, Parsons DS. Pediatric tracheobronchomalacia and major airway collapse. Ann Otol Rhinol Laryngol. 1992;101:300–309. - PubMed
-
- Boogaard R, Huijsmans SH, Pijnenburg MW, Tiddens HA, de Jongste JC, Merkus PJ. Tracheomalacia and bronchomalacia in children: incidence and patient characteristics. Chest. 2005;128:3391–3397. - PubMed
-
- Sotomayor JL, Godinez RI, Borden S, Wilmott RW. Large-airway collapse due to acquired tracheobronchomalacia in infancy. Am J Dis Child. 1986;140:367–371. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
