

Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study
- PMID: 28622955
- PMCID: PMC5537194
- DOI: 10.1016/S0140-6736(17)30770-5
Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study
Abstract
Background: Lifelong antiplatelet treatment is recommended after ischaemic vascular events, on the basis of trials done mainly in patients younger than 75 years. Upper gastrointestinal bleeding is a serious complication, but had low case fatality in trials of aspirin and is not generally thought to cause long-term disability. Consequently, although co-prescription of proton-pump inhibitors (PPIs) reduces upper gastrointestinal bleeds by 70-90%, uptake is low and guidelines are conflicting. We aimed to assess the risk, time course, and outcomes of bleeding on antiplatelet treatment for secondary prevention in patients of all ages.
Methods: We did a prospective population-based cohort study in patients with a first transient ischaemic attack, ischaemic stroke, or myocardial infarction treated with antiplatelet drugs (mainly aspirin based, without routine PPI use) after the event in the Oxford Vascular Study from 2002 to 2012, with follow-up until 2013. We determined type, severity, outcome (disability or death), and time course of bleeding requiring medical attention by face-to-face follow-up for 10 years. We estimated age-specific numbers needed to treat (NNT) to prevent upper gastrointestinal bleeding with routine PPI co-prescription on the basis of Kaplan-Meier risk estimates and relative risk reduction estimates from previous trials.
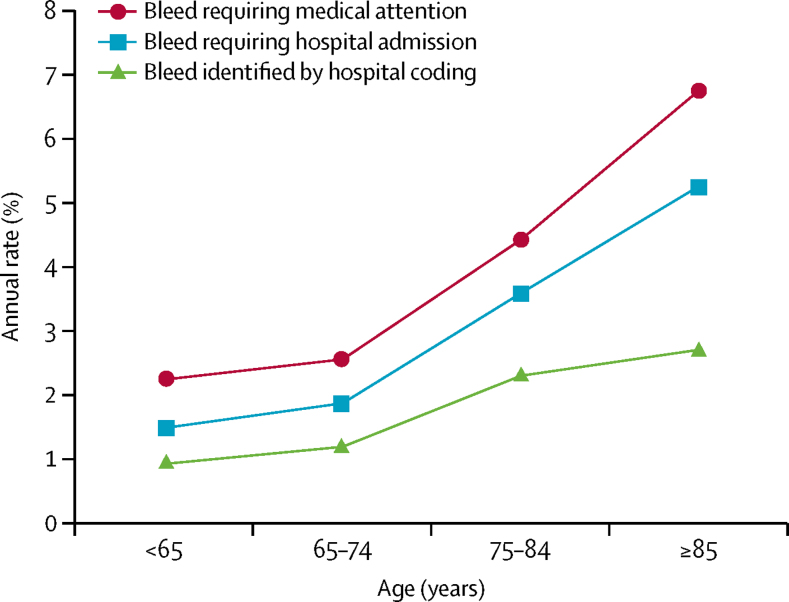
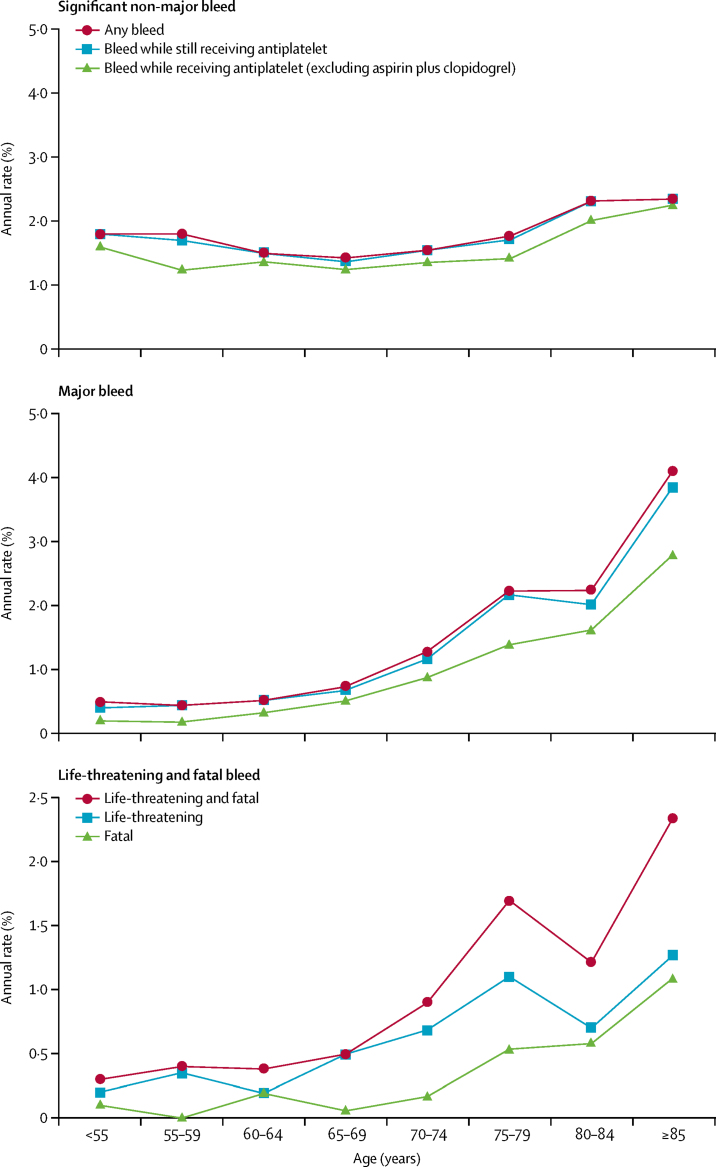
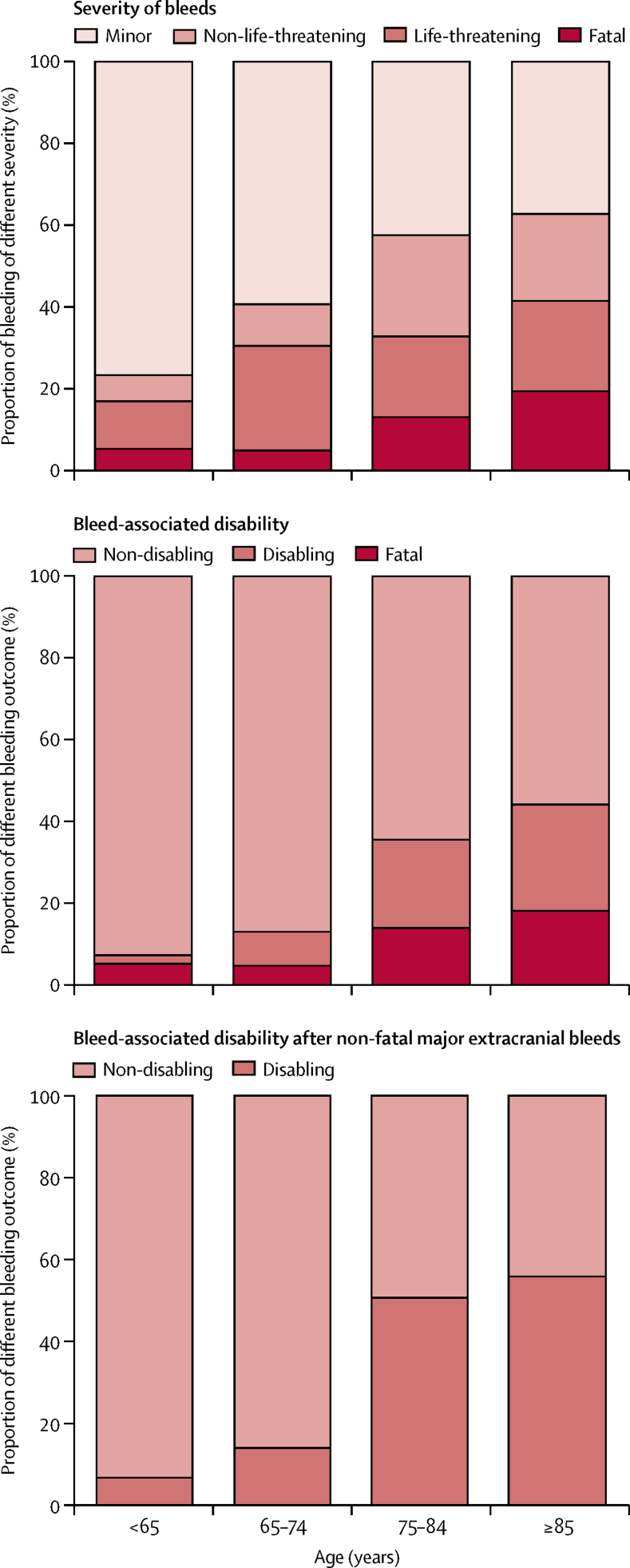
Findings: 3166 patients (1582 [50%] aged ≥75 years) had 405 first bleeding events (n=218 gastrointestinal, n=45 intracranial, and n=142 other) during 13 509 patient-years of follow-up. Of the 314 patients (78%) with bleeds admitted to hospital, 117 (37%) were missed by administrative coding. Risk of non-major bleeding was unrelated to age, but major bleeding increased steeply with age (≥75 years hazard ratio [HR] 3·10, 95% CI 2·27-4·24; p<0·0001), particularly for fatal bleeds (5·53, 2·65-11·54; p<0·0001), and was sustained during long-term follow-up. The same was true of major upper gastrointestinal bleeds (≥75 years HR 4·13, 2·60-6·57; p<0·0001), particularly if disabling or fatal (10·26, 4·37-24·13; p<0·0001). At age 75 years or older, major upper gastrointestinal bleeds were mostly disabling or fatal (45 [62%] of 73 patients vs 101 [47%] of 213 patients with recurrent ischaemic stroke), and outnumbered disabling or fatal intracerebral haemorrhage (n=45 vs n=18), with an absolute risk of 9·15 (95% CI 6·67-12·24) per 1000 patient-years. The estimated NNT for routine PPI use to prevent one disabling or fatal upper gastrointestinal bleed over 5 years fell from 338 for individuals younger than 65 years, to 25 for individuals aged 85 years or older.
Interpretation: In patients receiving aspirin-based antiplatelet treatment without routine PPI use, the long-term risk of major bleeding is higher and more sustained in older patients in practice than in the younger patients in previous trials, with a substantial risk of disabling or fatal upper gastrointestinal bleeding. Given that half of the major bleeds in patients aged 75 years or older were upper gastrointestinal, the estimated NNT for routine PPI use to prevent such bleeds is low, and co-prescription should be encouraged.
Funding: Wellcome Trust, Wolfson Foundation, British Heart Foundation, Dunhill Medical Trust, National Institute of Health Research (NIHR), and the NIHR Oxford Biomedical Research Centre.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Preventing major gastrointestinal bleeding in elderly patients.Lancet. 2017 Jul 29;390(10093):435-437. doi: 10.1016/S0140-6736(17)31507-6. Epub 2017 Jun 13. Lancet. 2017. PMID: 28622952 No abstract available.
-
Proton Pump Inhibitors may Reduce Bleeding Risk in Older Patients on Antiplatelet Therapy.Am J Nurs. 2017 Sep;117(9):56. doi: 10.1097/01.NAJ.0000524550.81437.76. Am J Nurs. 2017. PMID: 28837493 No abstract available.
-
Antiplatelet cessation to manage bleeding events in elderly people.Lancet. 2017 Dec 9;390(10112):2547-2548. doi: 10.1016/S0140-6736(17)33086-6. Epub 2017 Dec 8. Lancet. 2017. PMID: 29231833 No abstract available.
-
Is proton pump inhibitors' prophylaxis indicated for patients on antiplatelet therapy?Intern Emerg Med. 2018 Jun;13(4):585-587. doi: 10.1007/s11739-018-1827-9. Epub 2018 Mar 16. Intern Emerg Med. 2018. PMID: 29549551 No abstract available.
References
-
- Williams CD, Chan AT, Elman MR. Aspirin use among adults in the U.S. Results of a national survey. Am J Prev Med. 2015;48:501–508. - PubMed
-
- Elwood P, Morgan G, White J. Aspirin taking in a south Wales county. Br J Cardiol. 2011;18:238–240.
-
- Kernan WN, Ovbiagele B, Black HR. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:2160–2236. - PubMed
-
- Smith SC, Jr, Allen J, Blair SN. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation. 2006;113:2363–2372. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
