

Prevalence and treatment of atherogenic dyslipidemia in the primary prevention of cardiovascular disease in Europe: EURIKA, a cross-sectional observational study
- PMID: 28623902
- PMCID: PMC5473961
- DOI: 10.1186/s12872-017-0591-5
Prevalence and treatment of atherogenic dyslipidemia in the primary prevention of cardiovascular disease in Europe: EURIKA, a cross-sectional observational study
Abstract
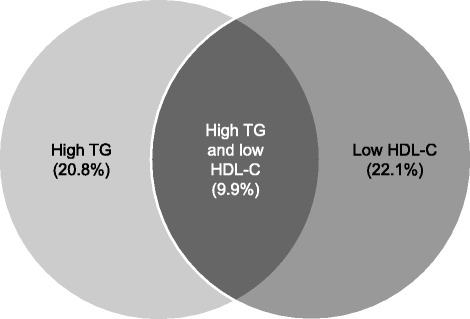
Background: Atherogenic dyslipidemia is associated with poor cardiovascular outcomes, yet markers of this condition are often ignored in clinical practice. Here, we address a clear evidence gap by assessing the prevalence and treatment of two markers of atherogenic dyslipidemia: elevated triglyceride levels and low levels of high-density lipoprotein cholesterol.
Methods: This cross-sectional observational study assessed the prevalence of two atherogenic dyslipidemia markers, high triglyceride levels and low high-density lipoprotein cholesterol levels, in the study population from the European Study on Cardiovascular Risk Prevention and Management in Usual Daily Practice (EURIKA; N = 7641; of whom 51.6% were female and 95.6% were White/Caucasian). The EURIKA population included European patients, aged at least 50 years with at least one cardiovascular risk factor but no history of cardiovascular disease.
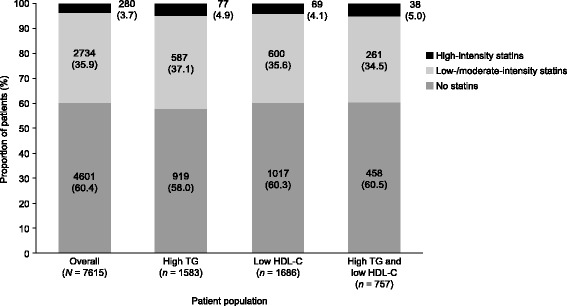
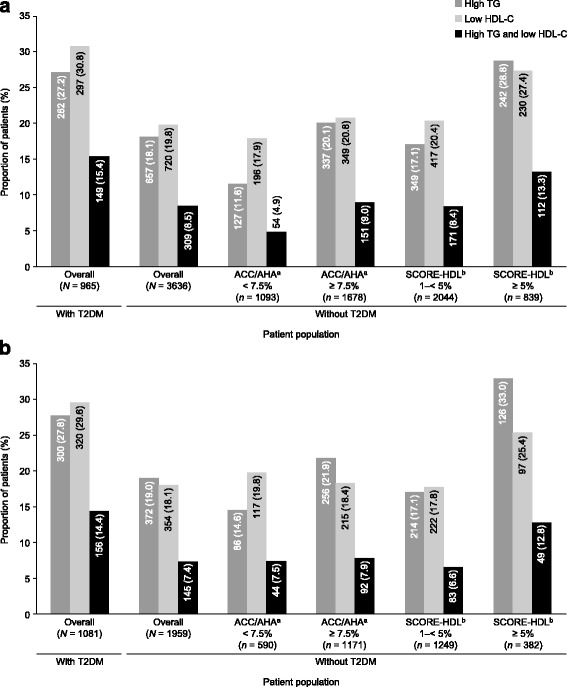
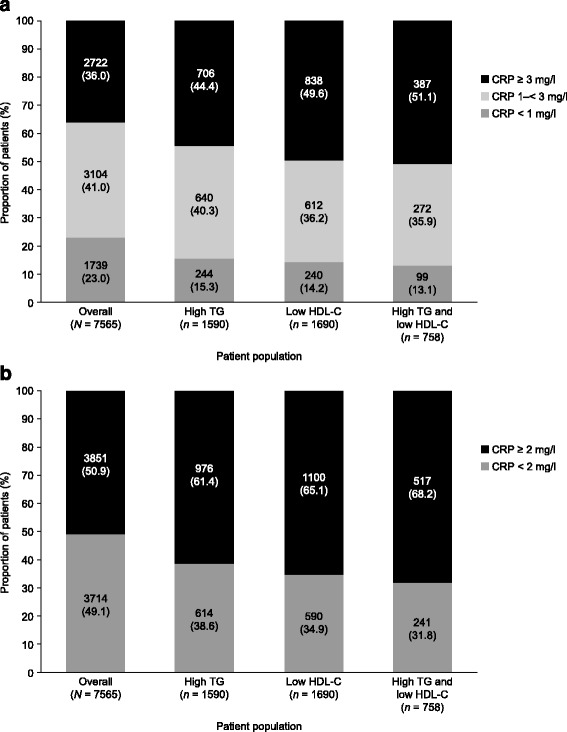
Results: Over 20% of patients from the EURIKA population have either triglyceride or high-density lipoprotein cholesterol levels characteristic of atherogenic dyslipidemia. Furthermore, the proportions of patients with one of these markers were higher in subpopulations with type 2 diabetes mellitus or those already calculated to be at high risk of cardiovascular disease. Approximately 55% of the EURIKA population who have markers of atherogenic dyslipidemia are not receiving lipid-lowering therapy.
Conclusions: A considerable proportion of patients with at least one major cardiovascular risk factor in the primary cardiovascular disease prevention setting have markers of atherogenic dyslipidemia. The majority of these patients are not receiving optimal treatment, as specified in international guidelines, and thus their risk of developing cardiovascular disease is possibly underestimated.
Trial registration: The present study is registered with ClinicalTrials.gov (ID: NCT00882336).
Keywords: Atherogenic dyslipidemia; Cardiovascular disease; Epidemiology; Risk factors/global assessment.
Figures
References
-
- European cardiovascular disease statistics http://www.ehnheart.org/cvd-statistics.html Accessed 18 Oct 2016.
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint Task Force of the European Society of Cardiology and Other Societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & rehabilitation (EACPR) Eur Heart J. 2016;37(29):2315–2381. doi: 10.1093/eurheartj/ehw106. - DOI - PMC - PubMed
-
- Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. ESC/EAS guidelines for the Management of Dyslipidaemias: the Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;253:281–344. - PubMed
-
- Chapman MJ, Ginsberg HN, Amarenco P, Andreotti F, Boren J, Catapano AL, et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur Heart J. 2011;32(11):1345–1361. doi: 10.1093/eurheartj/ehr112. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
