

Plasma proteome analysis in patients with pulmonary arterial hypertension: an observational cohort study
- PMID: 28624389
- PMCID: PMC5573768
- DOI: 10.1016/S2213-2600(17)30161-3
Plasma proteome analysis in patients with pulmonary arterial hypertension: an observational cohort study
Abstract
Background: Idiopathic and heritable pulmonary arterial hypertension form a rare but molecularly heterogeneous disease group. We aimed to measure and validate differences in plasma concentrations of proteins that are associated with survival in patients with idiopathic or heritable pulmonary arterial hypertension to improve risk stratification.
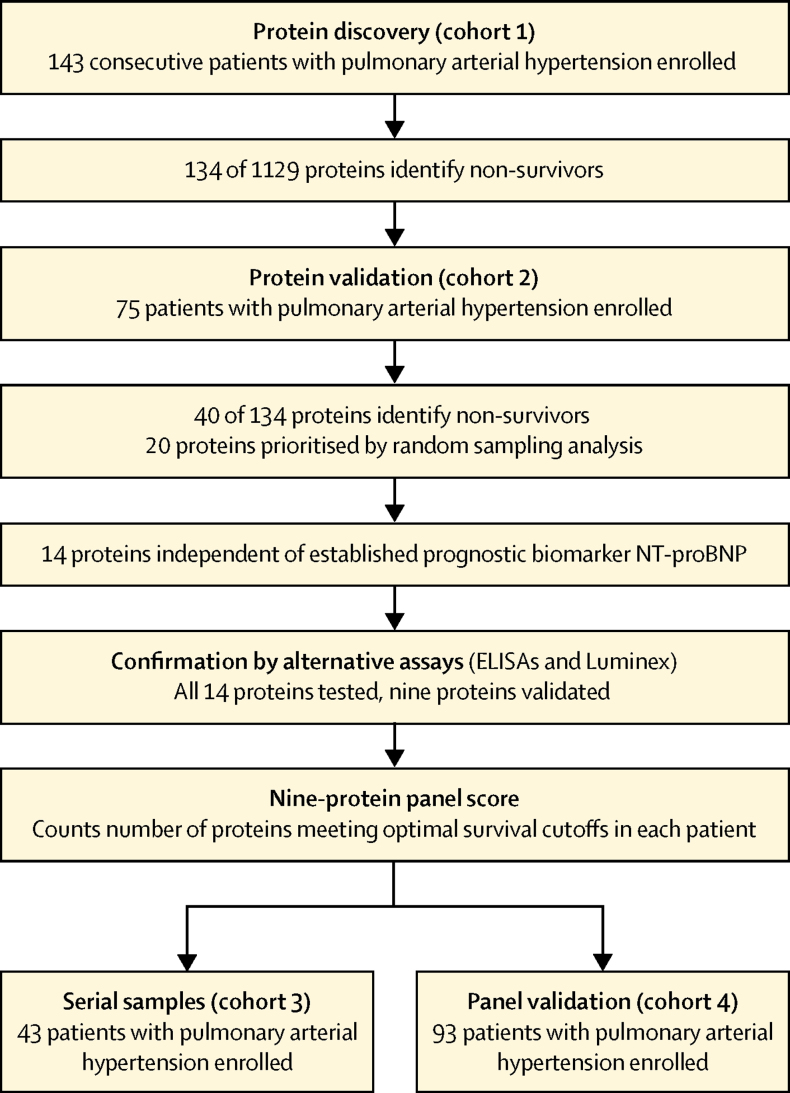
Methods: In this observational cohort study, we enrolled patients with idiopathic or heritable pulmonary arterial hypertension from London (UK; cohorts 1 and 2), Giessen (Germany; cohort 3), and Paris (France; cohort 4). Blood samples were collected at routine clinical appointment visits, clinical data were collected within 30 days of blood sampling, and biochemical data were collected within 7 days of blood sampling. We used an aptamer-based assay of 1129 plasma proteins, and patient clinical details were concealed to the technicians. We identified a panel of prognostic proteins, confirmed with alternative targeted assays, which we evaluated against the established prognostic risk equation for pulmonary arterial hypertension derived from the REVEAL registry. All-cause mortality was the primary endpoint.
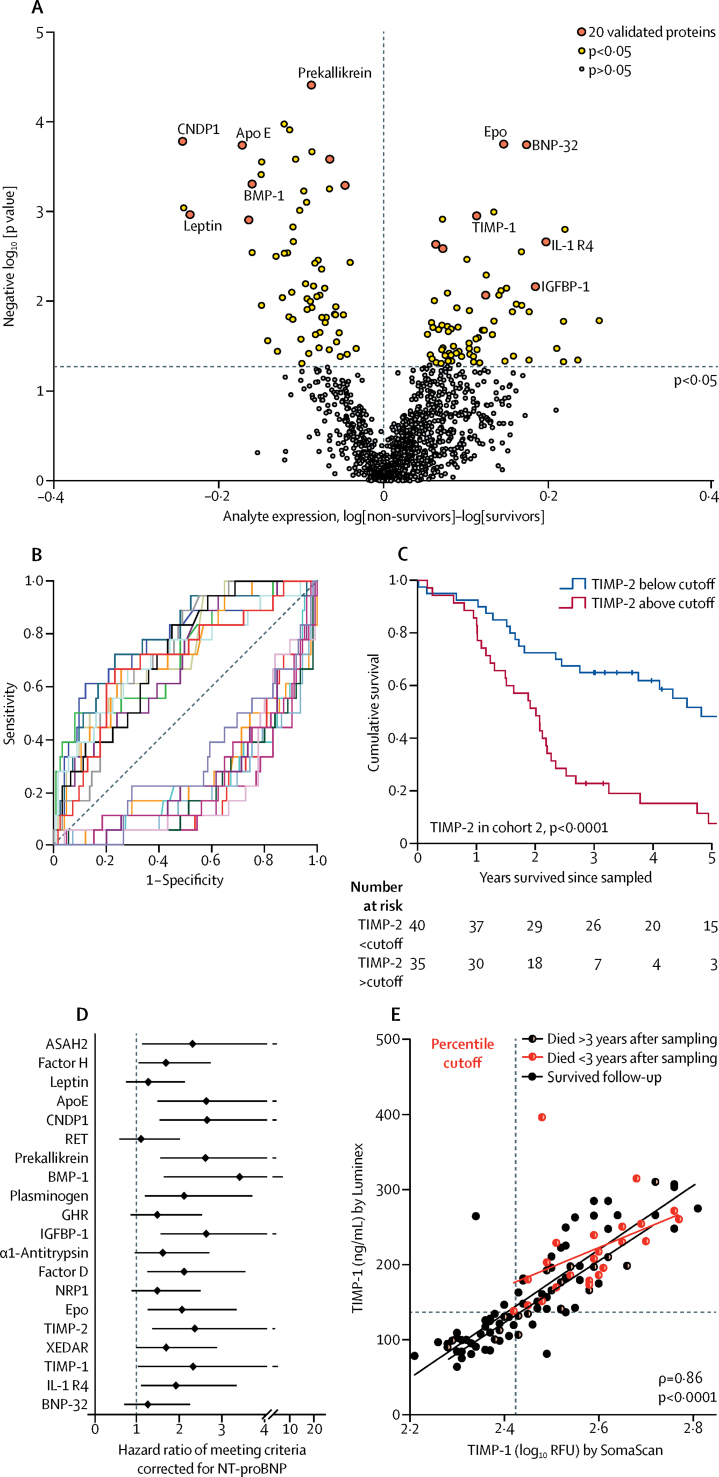
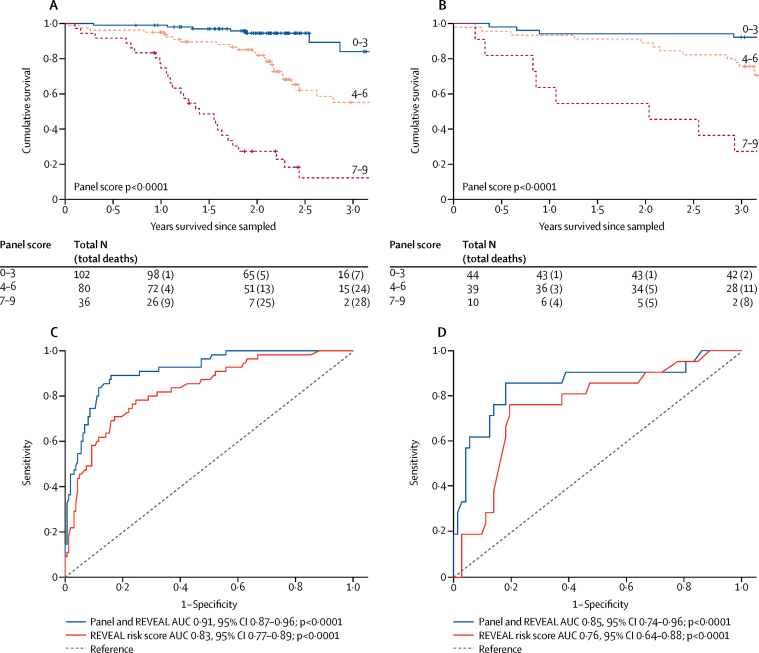
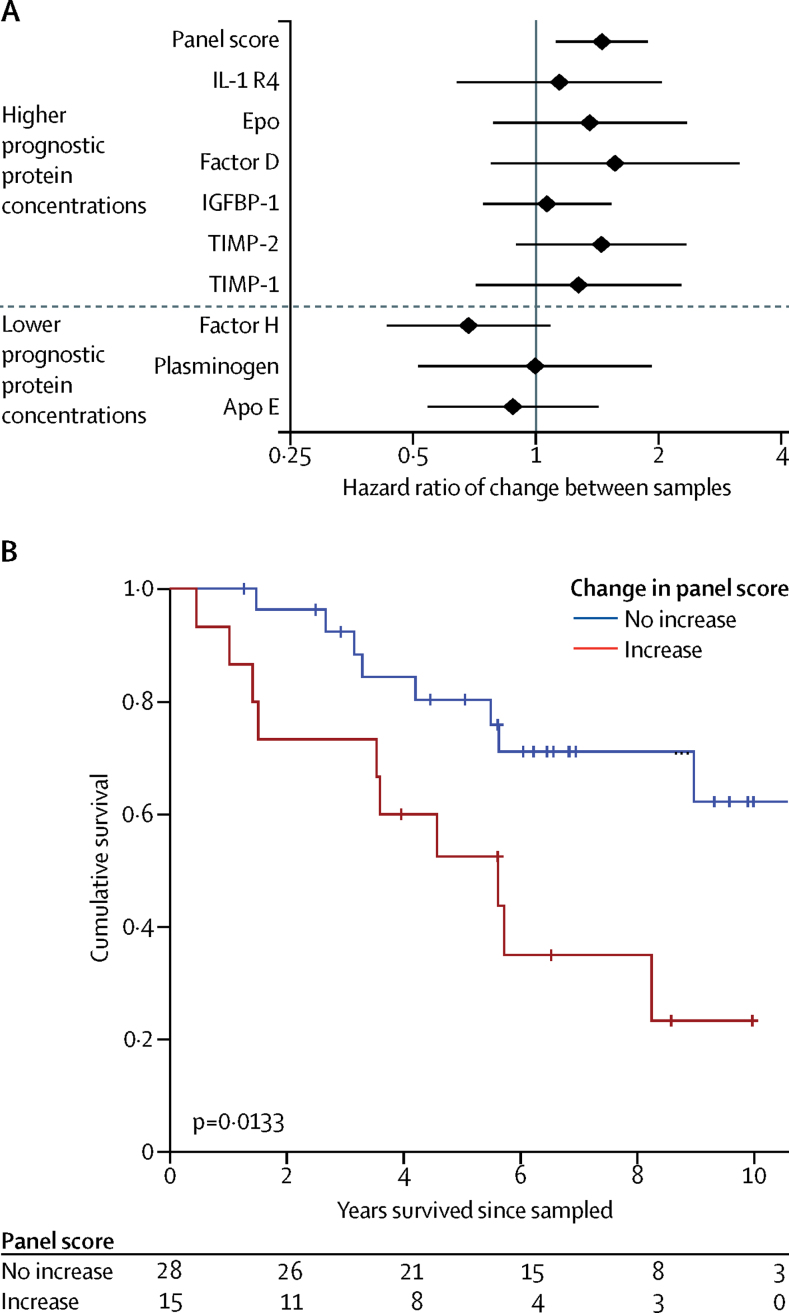
Findings: 20 proteins differentiated survivors and non-survivors in 143 consecutive patients with idiopathic or heritable pulmonary arterial hypertension with 2 years' follow-up (cohort 1) and in a further 75 patients with 2·5 years' follow-up (cohort 2). Nine proteins were both prognostic independent of plasma NT-proBNP concentrations and confirmed by targeted assays. The functions of these proteins relate to myocardial stress, inflammation, pulmonary vascular cellular dysfunction and structural dysregulation, iron status, and coagulation. A cutoff-based score using the panel of nine proteins provided prognostic information independent of the REVEAL equation, improving the C statistic from area under the curve 0·83 (for REVEAL risk score, 95% CI 0·77-0·89; p<0·0001) to 0·91 (for panel and REVEAL 0·87-0·96; p<0·0001) and improving reclassification indices without detriment to calibration. Poor survival was preceded by an adverse change in panel score in paired samples from 43 incident patients with pulmonary arterial hypertension in cohort 3 (p=0·0133). The protein panel was validated in 93 patients with idiopathic or heritable pulmonary arterial hypertension in cohort 4, with 4·4 years' follow-up and improved risk estimates, providing complementary information to the clinical risk equation.
Interpretation: A combination of nine circulating proteins identifies patients with pulmonary arterial hypertension with a high risk of mortality, independent of existing clinical assessments, and might have a use in clinical management and the evaluation of new therapies.
Funding: National Institute for Health Research, Wellcome Trust, British Heart Foundation, Assistance Publique-Hôpitaux de Paris, Inserm, Université Paris-Sud, and Agence Nationale de la Recherche.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 licence. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Aptamer-based proteomic profiling for prognostication in pulmonary arterial hypertension.Lancet Respir Med. 2017 Sep;5(9):671-672. doi: 10.1016/S2213-2600(17)30209-6. Epub 2017 Jun 15. Lancet Respir Med. 2017. PMID: 28624387 No abstract available.
References
-
- Humbert M, Sitbon O, Chaouat A. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–163. - PubMed
-
- McGoon MD, Benza RL, Escribano-Subias P. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(25 suppl):D51–D59. - PubMed
-
- Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest. 2012;142:448–456. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
