

Evaluation of hepatic fibrosis: a review from the society of abdominal radiology disease focus panel
- PMID: 28624924
- PMCID: PMC5994771
- DOI: 10.1007/s00261-017-1211-7
Evaluation of hepatic fibrosis: a review from the society of abdominal radiology disease focus panel
Abstract
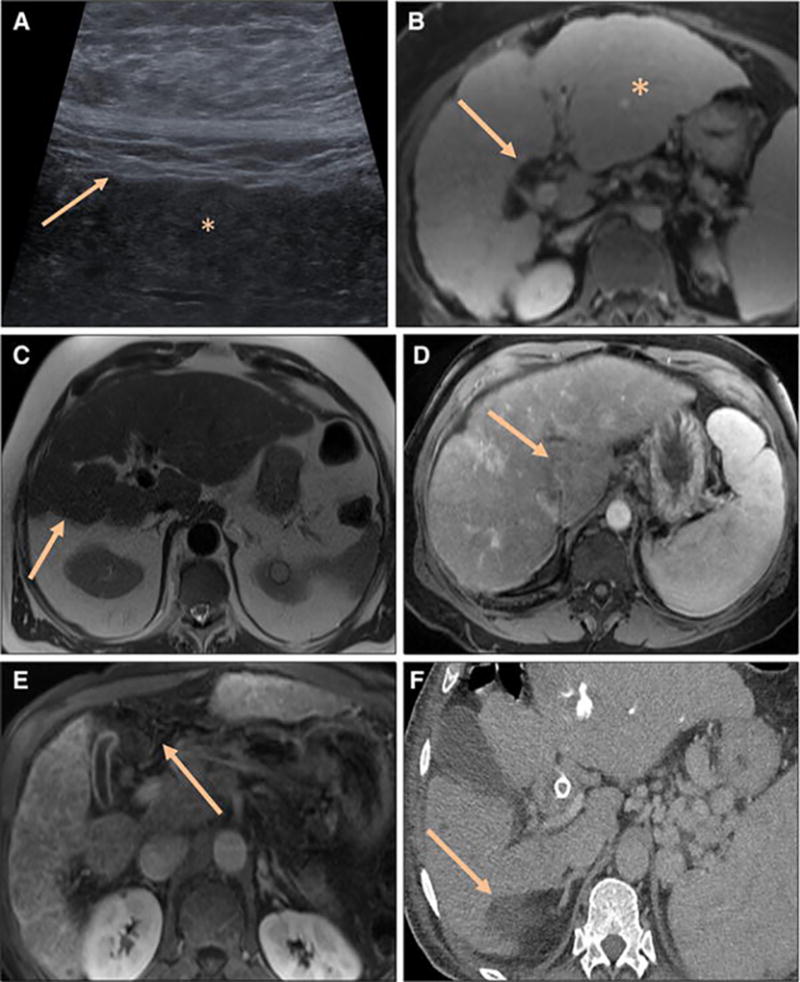
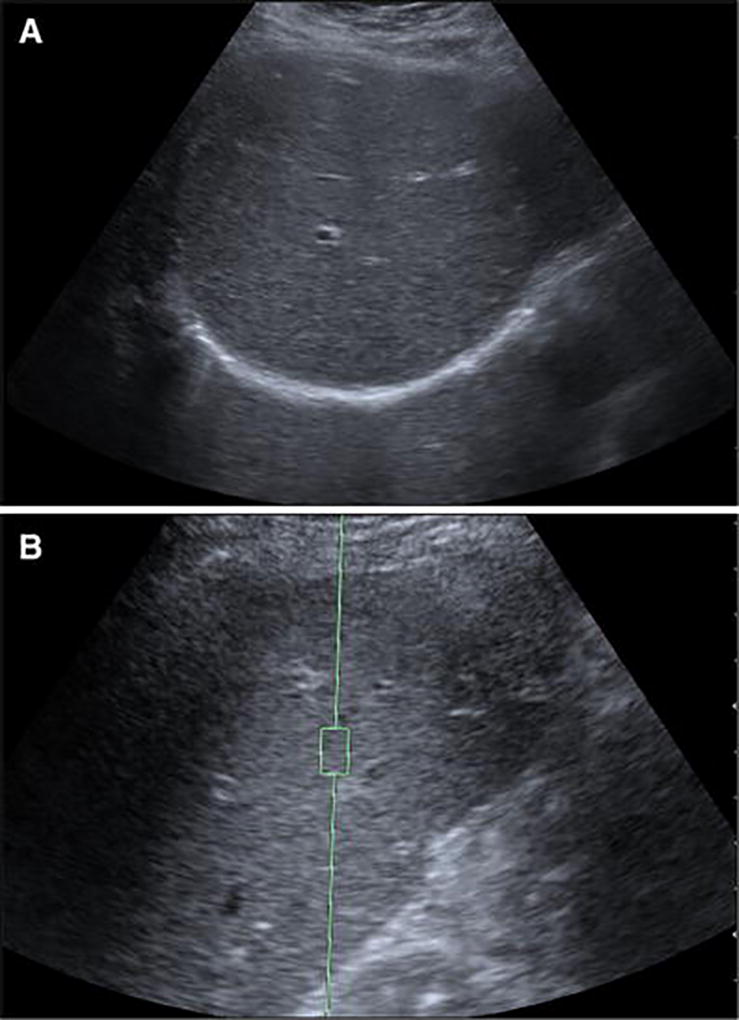
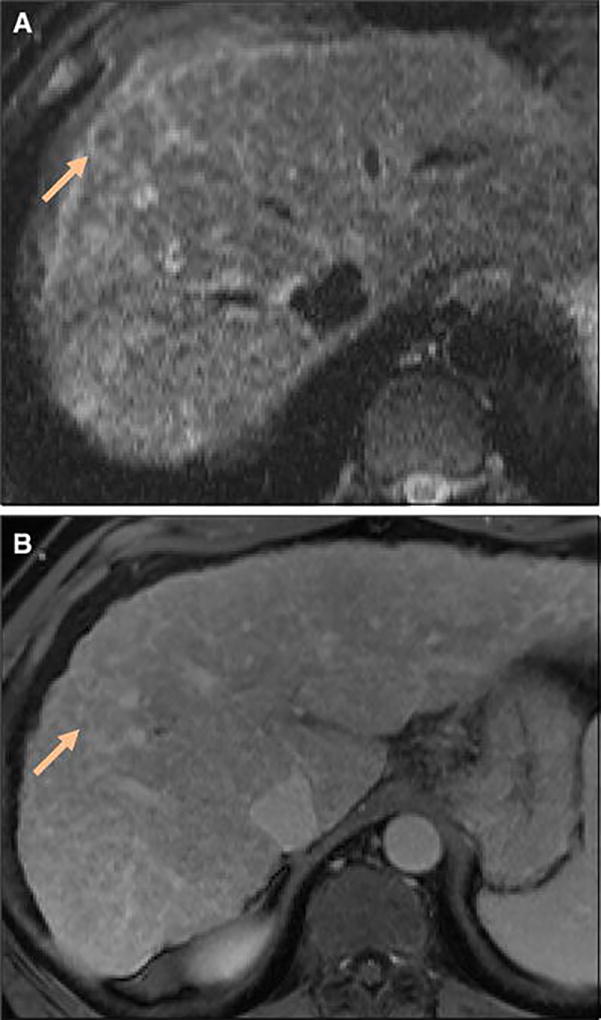
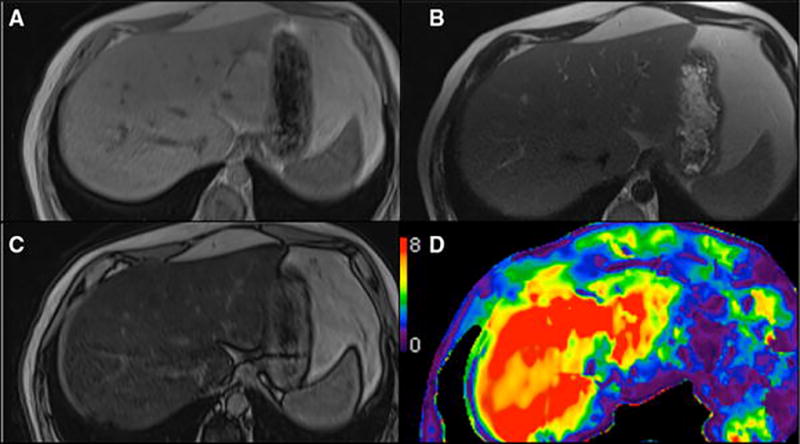
Hepatic fibrosis is potentially reversible; however early diagnosis is necessary for treatment in order to halt progression to cirrhosis and development of complications including portal hypertension and hepatocellular carcinoma. Morphologic signs of cirrhosis on ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI) alone are unreliable and are seen with more advanced disease. Newer imaging techniques to diagnose liver fibrosis are reliable and accurate, and include magnetic resonance elastography and US elastography (one-dimensional transient elastography and point shear wave elastography or acoustic radiation force impulse imaging). Research is ongoing with multiple other techniques for the noninvasive diagnosis of hepatic fibrosis, including MRI with diffusion-weighted imaging, hepatobiliary contrast enhancement, and perfusion; CT using perfusion, fractional extracellular space techniques, and dual-energy, contrast-enhanced US, texture analysis in multiple modalities, quantitative mapping, and direct molecular imaging probes. Efforts to advance the noninvasive imaging assessment of hepatic fibrosis will facilitate earlier diagnosis and improve patient monitoring with the goal of preventing the progression to cirrhosis and its complications.
Keywords: Chronic liver disease; Elastography; Fibrosis; Magnetic resonance imaging; Perfusion; Sonography.
Conflict of interest statement
Conflict of Interest:
Richard L. Ehman: RLE and the Mayo Clinic have intellectual property rights and a financial interest in MRE technology. RLE serves as CEO and holds equity in Resoundant, Inc.
Frank H. Miller MD has received a research grant from Siemens (no financial interest or funds).
Michael A. Ohliger has received research support from Gilead pharmaceuticals.
Bachir Taouli has received industry research grants from Guerbet and Bayer; is a consultant for Bioclinica, Median Technologies; and has received equipment support from Siemens.
The other authors including Jeanne M. Horowitz1, Sudhakar K. Venkatesh2, Kartik Jhaveri3, Patrick Kamath4, Anthony E. Samir6, Alvin C. Silva7, Michael S. Torbenson9, Michael L. Wells2, and Benjamin Yeh5 declare that they have no conflict of interest.
Figures
References
-
- Friedman SL. Liver fibrosis -- from bench to bedside. J Hepatol. 2003;38(Suppl 1):S38–53. - PubMed
-
- Shiffman ML, Stravitz RT, Contos MJ, Mills AS, Sterling RK, Luketic VA, Sanyal AJ, Cotterell A, Maluf D, Posner MP, Fisher RA. Histologic recurrence of chronic hepatitis C virus in patients after living donor and deceased donor liver transplantation. Liver Transpl. 2004;10(10):1248–1255. doi: 10.1002/lt.20232. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
