

Transpulmonary thermodilution: advantages and limits
- PMID: 28625165
- PMCID: PMC5474867
- DOI: 10.1186/s13054-017-1739-5
Transpulmonary thermodilution: advantages and limits
Abstract
Background: For complex patients in the intensive care unit or in the operating room, many questions regarding their haemodynamic management cannot be answered with simple clinical examination. In particular, arterial pressure allows only a rough estimation of cardiac output. Transpulmonary thermodilution is a technique that provides a full haemodynamic assessment through cardiac output and other indices.
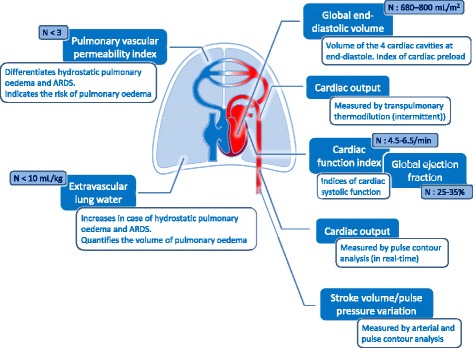
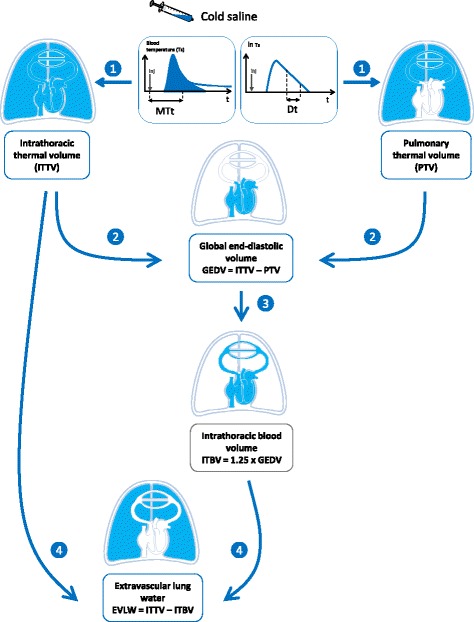
Main body: Through the analysis of the thermodilution curve recorded at the tip of an arterial catheter after the injection of a cold bolus in the venous circulation, transpulmonary thermodilution intermittently measures cardiac output. This measure allows the calibration of pulse contour analysis. This provides continuous and real time monitoring of cardiac output, which is not possible with the pulmonary artery catheter. Transpulmonary thermodilution provides several variables beyond cardiac output. It estimates the end-diastolic volume of the four cardiac cavities, which is a marker of cardiac preload. It provides an estimation of the systolic function of the combined ventricles. It is more direct than the pulmonary artery catheter, but does not allow the distinct estimation of right and left cardiac function. It is easier and faster to perform than echocardiography, but does not provide a full evaluation of the cardiac structure and function. Transpulmonary thermodilution has the unique advantage of being able to estimate at the bedside extravascular lung water, which quantifies the volume of pulmonary oedema, and pulmonary vascular permeability, which quantifies the degree of a pulmonary capillary leak. Both indices are helpful for guiding fluid strategy, especially in case of acute respiratory distress syndrome.
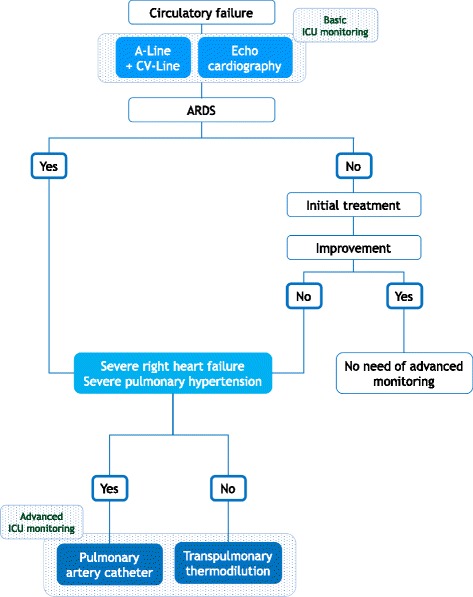
Conclusions: Transpulmonary thermodilution provides a full cardiovascular evaluation that allows one to answer many questions regarding haemodynamic management. It belongs to the category of "advanced" devices that are indicated for the most critically ill and/or complex patients.
Keywords: Cardiac output; Cardiac preload; Extravascular lung water; Fluid responsiveness; Haemodynamic monitoring.
Figures
Comment in
-
Main limitations of transpulmonary thermodilution: set targets.Crit Care. 2017 Sep 18;21(1):242. doi: 10.1186/s13054-017-1833-8. Crit Care. 2017. PMID: 28923088 Free PMC article. No abstract available.
References
-
- Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1795–815. doi: 10.1007/s00134-014-3525-z. - DOI - PMC - PubMed
-
- Stetz CW, Miller RG, Kelly GE, Raffin TA. Reliability of the thermodilution method in the determination of cardiac output in clinical practice. Am Rev Respir Dis. 1982;126(6):1001–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
