

IgG-specific cell-based assay detects potentially pathogenic MuSK-Abs in seronegative MG
- PMID: 28626780
- PMCID: PMC5459793
- DOI: 10.1212/NXI.0000000000000357
IgG-specific cell-based assay detects potentially pathogenic MuSK-Abs in seronegative MG
Abstract
Objective: To increase the detection of MuSK-Abs using a CBA and test their pathogenicity.
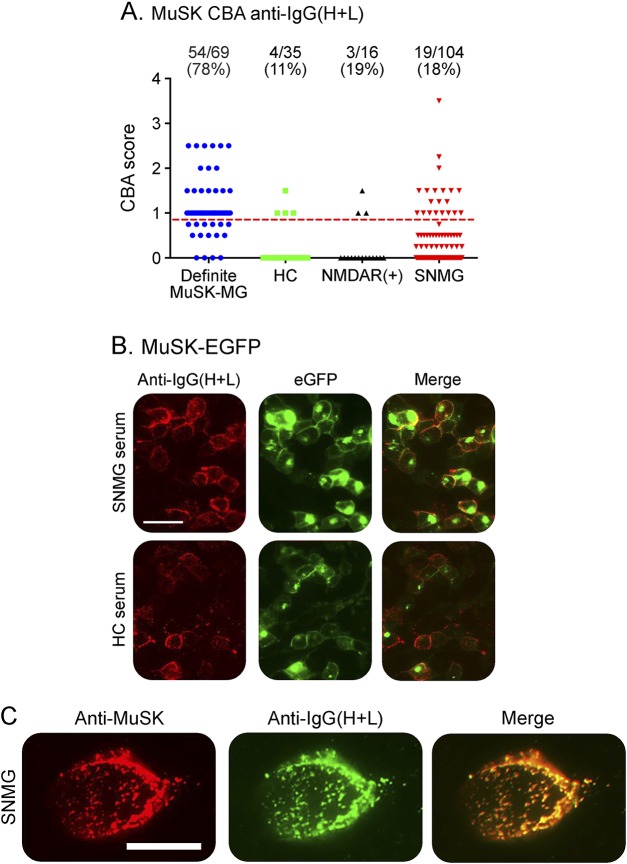
Methods: Sera from 69 MuSK-RIA-positive patients with myasthenia gravis (MG) (Definite MuSK-MG), 169 patients negative for MuSK-RIA and AChR-RIA (seronegative MG, SNMG), 35 healthy individuals (healthy controls, HCs), and 16 NMDA receptor-Ab-positive (NMDAR-Ab) disease controls were tested for binding to MuSK on a CBA using different secondary antibodies.
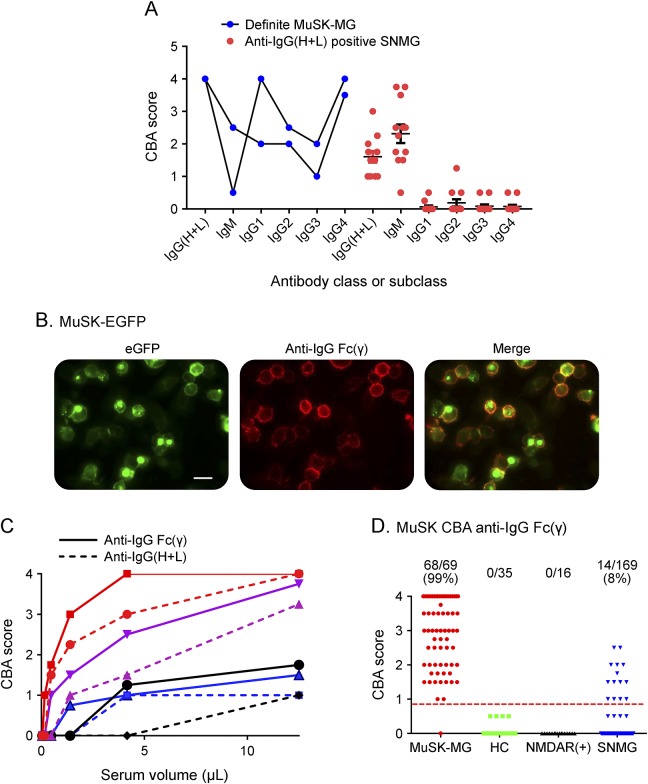
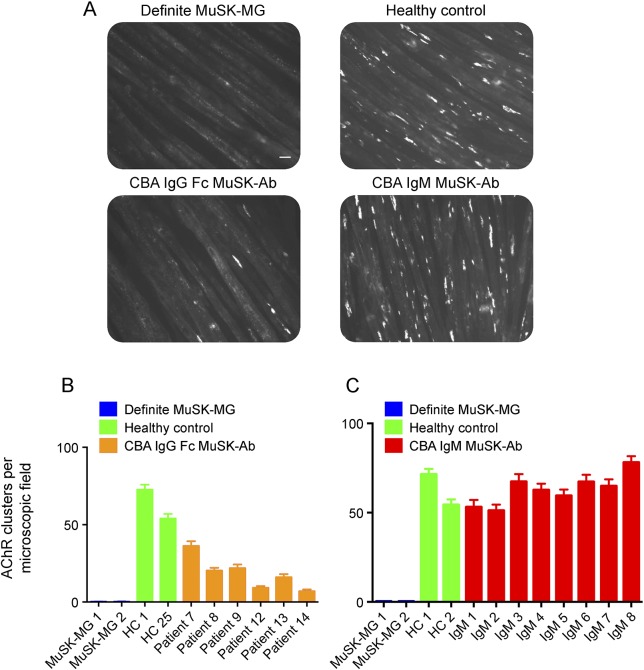
Results: Initially, in addition to 18% of SNMG sera, 11% of HC and 19% of NMDAR-Ab sera showed positive binding to MuSK-transfected cells; this low specificity was due to anti-IgG(H+L) detection of IgM bound nonspecifically to MuSK. Using an IgG Fc gamma-specific secondary antibody, MuSK-Abs were detected by CBA in 68/69 (99%) of Definite MuSK-MG, 0/35 HCs, 0/16 NMDAR-Ab, and 14/169 (8%) of SNMG sera, providing increased sensitivity with high specificity. The RIA-negative, CBA-positive MuSK-IgG sera, but not IgM-MuSK-binding sera, reduced agrin-induced AChR clustering in C2C12 myotubes, qualitatively similar to RIA-positive MuSK-Abs.
Conclusions: An IgG-specific MuSK-CBA can reliably detect IgG MuSK-Abs and increase sensitivity. In the MuSK-CBA, IgG specificity is essential. The positive sera demonstrated pathogenic potential in the in vitro AChR-clustering assay, although less effective than Definite MuSK-MG sera, and the patients had less severe clinical disease. Use of IgG-specific secondary antibodies may improve the results of other antibody tests.
Classification of evidence: This study provides Class III evidence that an IgG-specific MuSK-CBA identifies patients with MG.
Figures
References
-
- Waters P, Pettinghill P, Lang B. Detection methods for neural antibodies. In: Pittock S, Vincent A, editors. Autoimmune Neurology. Amsterdam: Elsevier; 2016:147–163. - PubMed
-
- Jacob S, Viegas S, Leite MI, et al. . Presence and pathogenic relevance of antibodies to clustered acetylcholine receptor in ocular and generalised myasthenia gravis. Arch Neurol 2012;69:994–1001. - PubMed
-
- Devic P, Petiot P, Simonet T, et al. . Antibodies to clustered acetylcholine receptor: expanding the phenotype. Eur J Neurol 2014;21:130–134. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials