

Epigenetics, inflammation and metabolism in right heart failure associated with pulmonary hypertension
- PMID: 28628000
- PMCID: PMC5841893
- DOI: 10.1177/2045893217714463
Epigenetics, inflammation and metabolism in right heart failure associated with pulmonary hypertension
Abstract
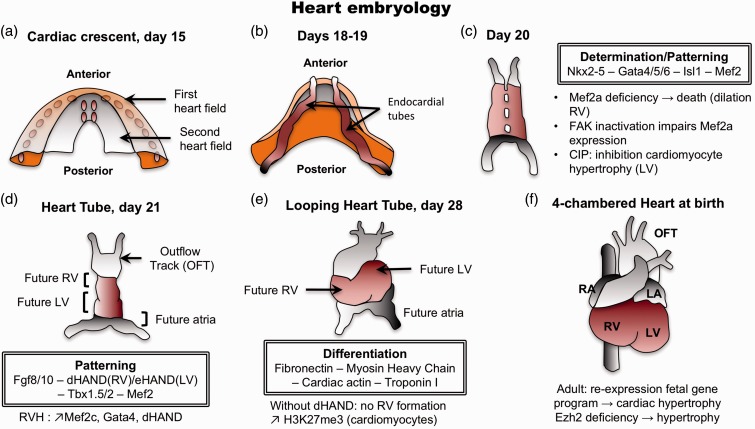
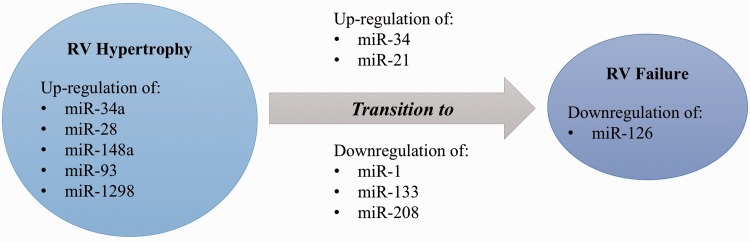
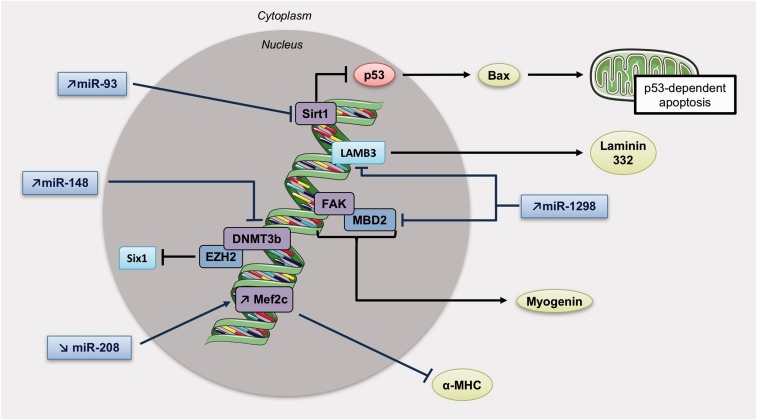
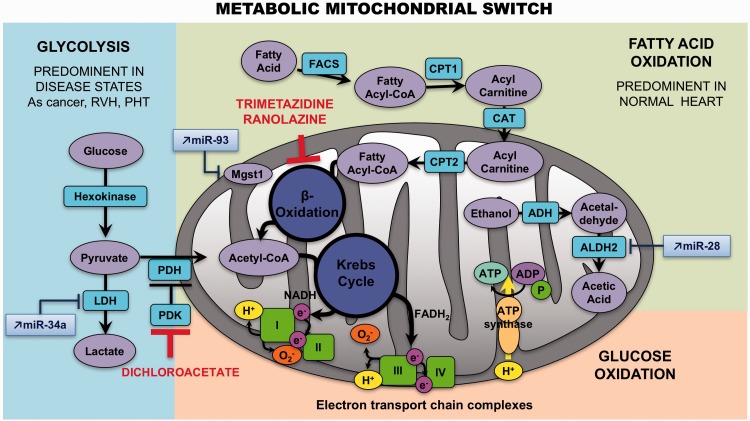
Right ventricular failure (RVF) is the most important prognostic factor for both morbidity and mortality in pulmonary arterial hypertension (PAH), but also occurs in numerous other common diseases and conditions, including left ventricle dysfunction. RVF remains understudied compared with left ventricular failure (LVF). However, right and left ventricles have many differences at the morphological level or the embryologic origin, and respond differently to pressure overload. Therefore, knowledge from the left ventricle cannot be extrapolated to the right ventricle. Few studies have focused on the right ventricle and have permitted to increase our knowledge on the right ventricular-specific mechanisms driving decompensation. Here we review basic principles such as mechanisms accounting for right ventricle hypertrophy, dysfunction, and transition toward failure, with a focus on epigenetics, inflammatory, and metabolic processes.
Keywords: cytokines; mitochondrial switch; right ventricle hypertrophy.
Figures
References
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009; 119(16): 2250–2294. - PubMed
-
- Bogaard HJ, Abe K, Vonk Noordegraaf A, et al. The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest 2009; 135(3): 794–804. - PubMed
-
- Haddad F, Doyle R, Murphy DJ, et al. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 2008; 117(13): 1717–1731. - PubMed
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol 2013; 62(25 Suppl): D22–33. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
