

Hospital readmission within 10 years post stroke: frequency, type and timing
- PMID: 28629340
- PMCID: PMC5477341
- DOI: 10.1186/s12883-017-0897-z
Hospital readmission within 10 years post stroke: frequency, type and timing
Abstract
Background: The aim of this study was to examine the hospital readmissions in a 10 year follow-up of a stroke cohort previously studied for acute and subacute complications and to focus on their frequency, their causes and their timing.
Methods: The hospital records of 243 patients, 50% of a cohort of 489 patients acutely and consecutively admitted to our stroke unit in 2002/3, were subjected to review 10 years after the incidental stroke and all acute admissions were examined. The main admitting diagnoses were attributed to one of 18 predefined categories of illness. Additionally, the occurrence of death was registered.
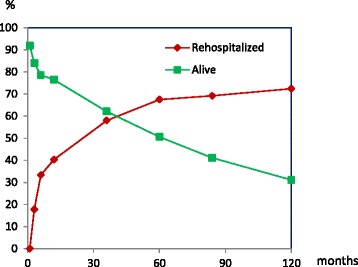
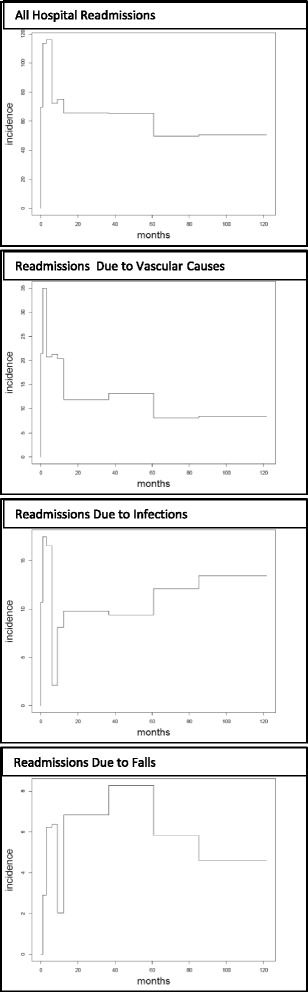
Results: After 10 years 68.9% of patients had died and 72.4% had been readmitted to the hospital with a mean number of readmissions of 3.4 (+15.1 SD). 20% of the readmissions were due to a vascular cause, 17.3% were caused by infection, 9.3% by falls with (6.1%) and without fracture, 5.7% by a hemorrhagic event. The readmission rate was highest in the first 6 months post stroke with a rate of 116.2 admissions/100 live patient-years. Falls with fractures occurred maximally 3-5 years post stroke.
Conclusions: Hospital readmissions over the 10 years following stroke are caused by vascular events, infections, falls and hemorrhagic events, where the first 6 months are a period of particular vulnerability. The magnitude and the spectrum of these long-term complications suggest the need for a more comprehensive approach to post stroke prophylaxis.
Keywords: Longterm follow-up; Readmission; Readmission rate; Secondary prophylaxis; Stroke.
Figures
References
-
- Lewsey J, Ebueku O, Jhund PS, et al. Temporal trends and risk factors for readmission for infections, gastrointestinal and immobility complications after an incident hospitalisation for stroke in Scotland between 1997 and 2005. BMC Neurol. 2015;15:3. doi: 10.1186/s12883-014-0257-1. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
