

Trajectories of Emergent Central Sleep Apnea During CPAP Therapy
- PMID: 28629918
- PMCID: PMC6026232
- DOI: 10.1016/j.chest.2017.06.010
Trajectories of Emergent Central Sleep Apnea During CPAP Therapy
Abstract
Background: The emergence of central sleep apnea (CSA) during positive airway pressure (PAP) therapy has been observed clinically in approximately 10% of obstructive sleep apnea titration studies. This study assessed a PAP database to investigate trajectories of treatment-emergent CSA during continuous PAP (CPAP) therapy.
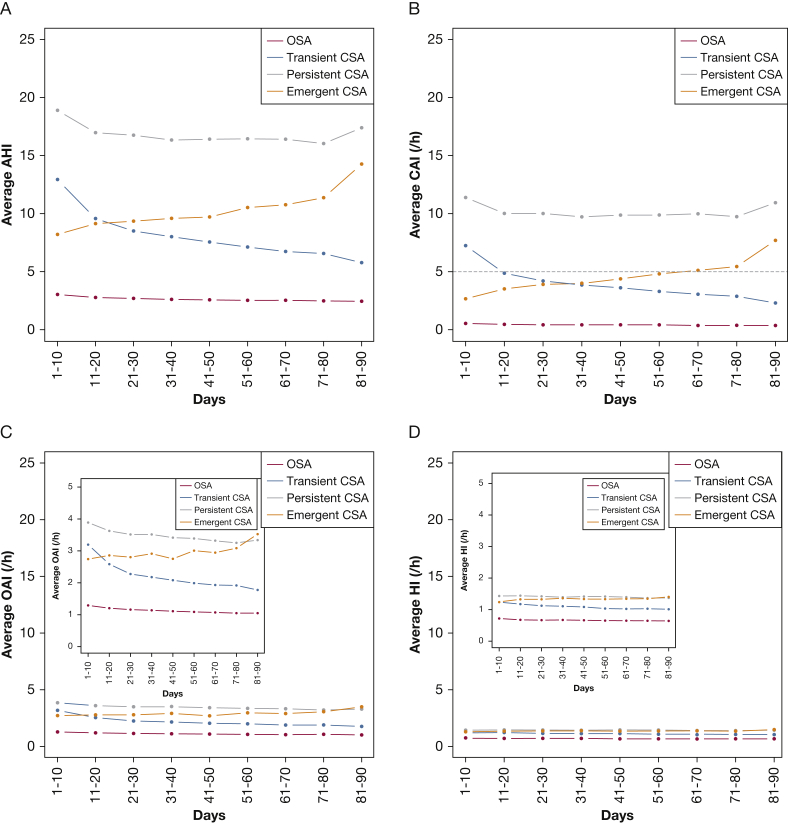
Methods: U.S. telemonitoring device data were analyzed for the presence/absence of emergent CSA at baseline (week 1) and week 13. Defined groups were as follows: obstructive sleep apnea (average central apnea index [CAI] < 5/h in week 1, < 5/h in week 13); transient CSA (CAI ≥ 5/h in week 1, < 5/h in week 13); persistent CSA (CAI ≥ 5/h in week 1, ≥ 5/h in week 13); emergent CSA (CAI < 5/h in week 1, ≥ 5/h in week 13).
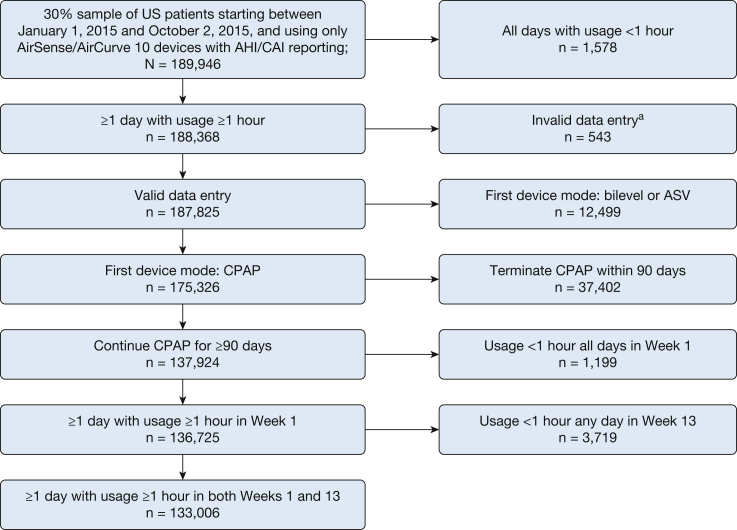
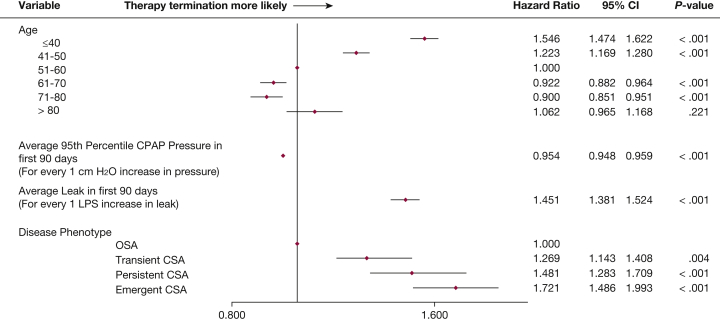
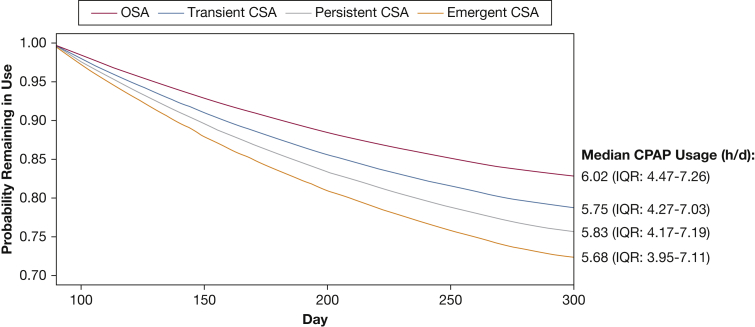
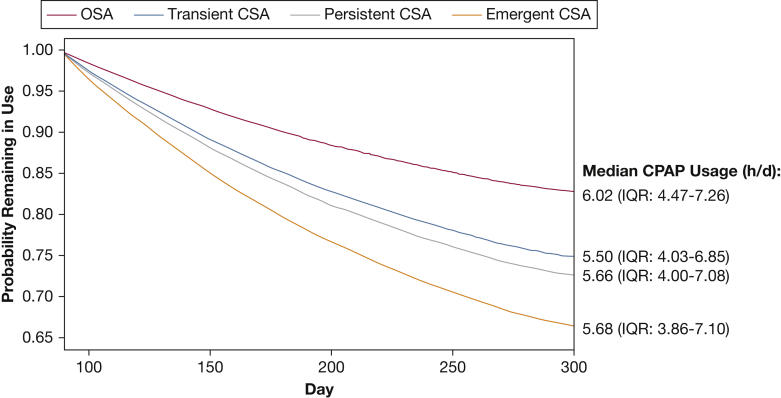
Results: Patients (133,006) used CPAP for ≥ 90 days and had ≥ 1 day with use of ≥ 1 h in week 1 and week 13. The proportion of patients with CSA in week 1 or week 13 was 3.5%; of these, CSA was transient, persistent, or emergent in 55.1%, 25.2%, and 19.7%, respectively. Patients with vs without treatment-emergent CSA were older, had higher residual apnea-hypopnea index and CAI at week 13, and more leaks (all P < .001). Patients with any treatment-emergent CSA were at higher risk of therapy termination vs those who did not develop CSA (all P < .001).
Conclusions: Our study identified a variety of CSA trajectories during CPAP therapy, identifying several different clinical phenotypes. Identification of treatment-emergent CSA by telemonitoring could facilitate early intervention to reduce the risk of therapy discontinuation and shift to more efficient ventilator modalities.
Keywords: CPAP; central sleep apnea; telemonitoring.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Central sleep apnea during continuous positive airway pressure therapy in obstructive sleep apnea patients: from the compliance to adaptation, maladaptation and reflexes.J Thorac Dis. 2017 Nov;9(11):4152-4156. doi: 10.21037/jtd.2017.09.116. J Thorac Dis. 2017. PMID: 29268457 Free PMC article. No abstract available.
-
Emergent central sleep apnea during CPAP therapy-clinical implications.J Thorac Dis. 2017 Nov;9(11):4182-4184. doi: 10.21037/jtd.2017.09.131. J Thorac Dis. 2017. PMID: 29268465 Free PMC article. No abstract available.
References
-
- Westhoff M., Arzt M., Litterst P. Prevalence and treatment of central sleep apnoea emerging after initiation of continuous positive airway pressure in patients with obstructive sleep apnoea without evidence of heart failure. Sleep Breath. 2012;16(1):71–78. - PubMed
-
- American Academy of Sleep Medicine . 3rd ed. American Academy of Sleep Medicine; Darien, IL: 2014. International Classification of Sleep Disorders.
-
- Randerath W., Verbraecken J., Andreas S. Definition, discrimination, diagnosis and treatment of central breathing disorders during sleep. Eur Respir J. 2017;49(1):1600959. - PubMed
-
- Verbraecken J. Complex sleep apnoea syndrome. Breathe. 2013;9(5):373–380.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
