

Childhood Firearm Injuries in the United States
- PMID: 28630118
- PMCID: PMC6488039
- DOI: 10.1542/peds.2016-3486
Childhood Firearm Injuries in the United States
Erratum in
-
Fowler KA, Dahlberg LL, Haileyesus T, et al. Childhood Firearm Injuries in the United States. Pediatrics. 2017;140(1):e20163486.Pediatrics. 2017 Oct;140(4):e20172298. doi: 10.1542/peds.2017-2298. Pediatrics. 2017. PMID: 28970344 No abstract available.
Abstract
Objectives: Examine fatal and nonfatal firearm injuries among children aged 0 to 17 in the United States, including intent, demographic characteristics, trends, state-level patterns, and circumstances.
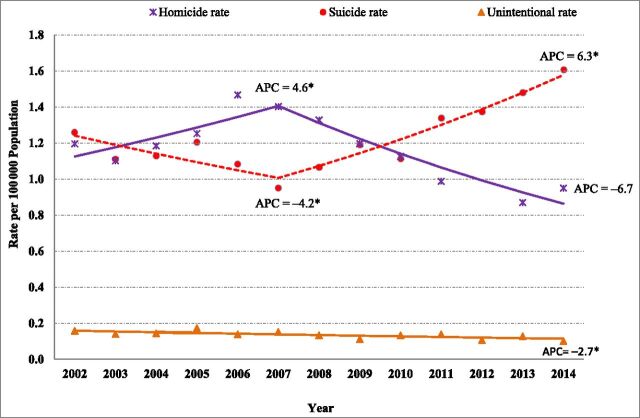
Methods: Fatal injuries were examined by using data from the National Vital Statistics System and nonfatal injuries by using data from the National Electronic Injury Surveillance System. Trends from 2002 to 2014 were tested using joinpoint regression analyses. Incident characteristics and circumstances were examined by using data from the National Violent Death Reporting System.
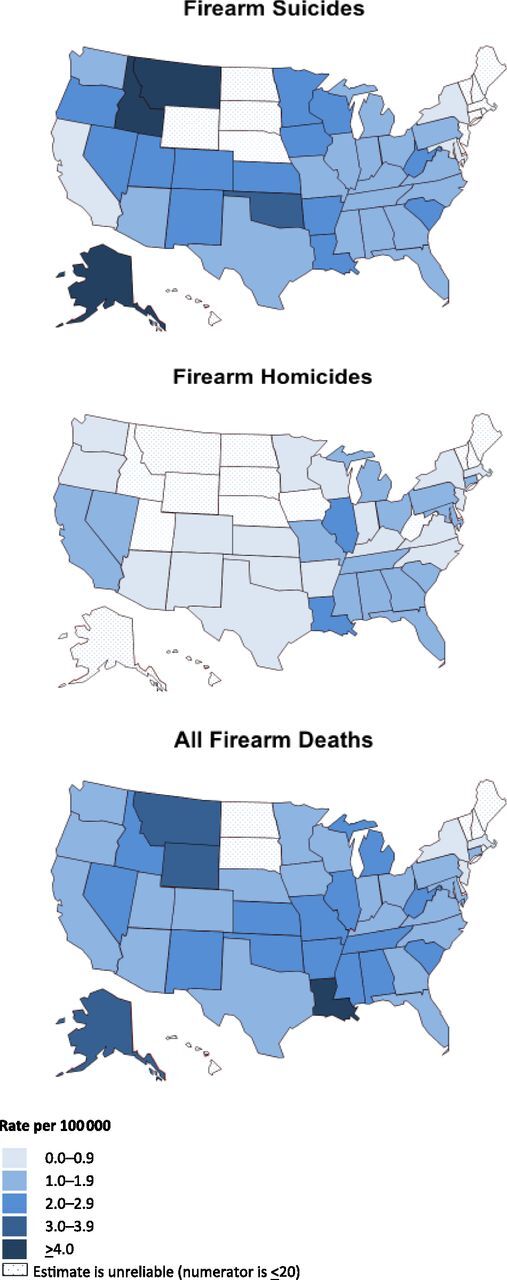
Results: Nearly 1300 children die and 5790 are treated for gunshot wounds each year. Boys, older children, and minorities are disproportionately affected. Although unintentional firearm deaths among children declined from 2002 to 2014 and firearm homicides declined from 2007 to 2014, firearm suicides decreased between 2002 and 2007 and then showed a significant upward trend from 2007 to 2014. Rates of firearm homicide among children are higher in many Southern states and parts of the Midwest relative to other parts of the country. Firearm suicides are more dispersed across the United States with some of the highest rates occurring in Western states. Firearm homicides of younger children often occurred in multivictim events and involved intimate partner or family conflict; older children more often died in the context of crime and violence. Firearm suicides were often precipitated by situational and relationship problems. The shooter playing with a gun was the most common circumstance surrounding unintentional firearm deaths of both younger and older children.
Conclusions: Firearm injuries are an important public health problem, contributing substantially to premature death and disability of children. Understanding their nature and impact is a first step toward prevention.
Copyright © 2017 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Comment in
-
Confronting the Firearm Injury Plague.Pediatrics. 2017 Jul;140(1):e20171300. doi: 10.1542/peds.2017-1300. Epub 2017 Jun 19. Pediatrics. 2017. PMID: 28630117 No abstract available.
References
-
- Finkelhor D, Turner HA, Shattuck A, Hamby SL. Prevalence of childhood exposure to violence, crime, and abuse: results from the national survey of children’s exposure to violence. JAMA Pediatr. 2015;169(8):746–754 - PubMed
-
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control . Web-based injury statistics query and reporting system (WISQARS). 2005. Available at: www.cdc.gov/injury/wisqars. Accessed October 2, 2016
-
- Leventhal JM, Gaither JR, Sege R. Hospitalizations due to firearm injuries in children and adolescents. Pediatrics. 2014;133(2):219–225 - PubMed
-
- DiScala C, Sege R. Outcomes in children and young adults who are hospitalized for firearms-related injuries. Pediatrics. 2004;113(5):1306–1312 - PubMed
-
- Srinivasan S, Mannix R, Lee LK. Epidemiology of paediatric firearm injuries in the USA, 2001-2010. Arch Dis Child. 2014;99(4):331–335 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
