

Distinctive pathological and clinical features of lung carcinoids with high proliferation index
- PMID: 28631159
- PMCID: PMC5711990
- DOI: 10.1007/s00428-017-2177-0
Distinctive pathological and clinical features of lung carcinoids with high proliferation index
Abstract
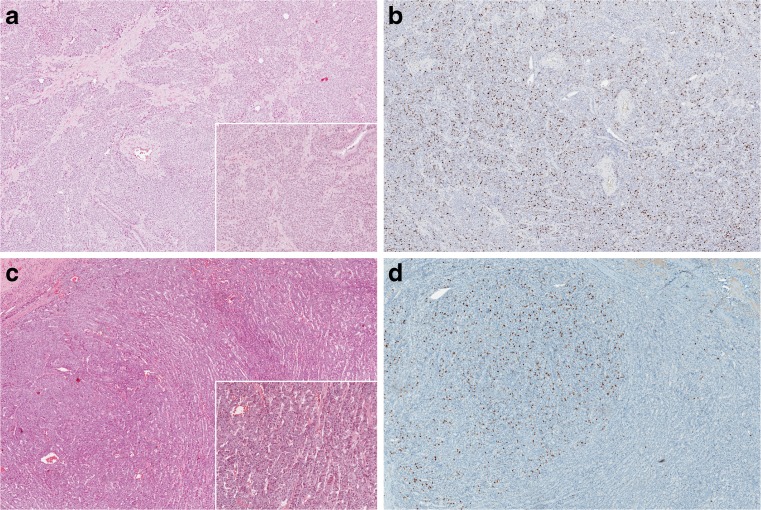
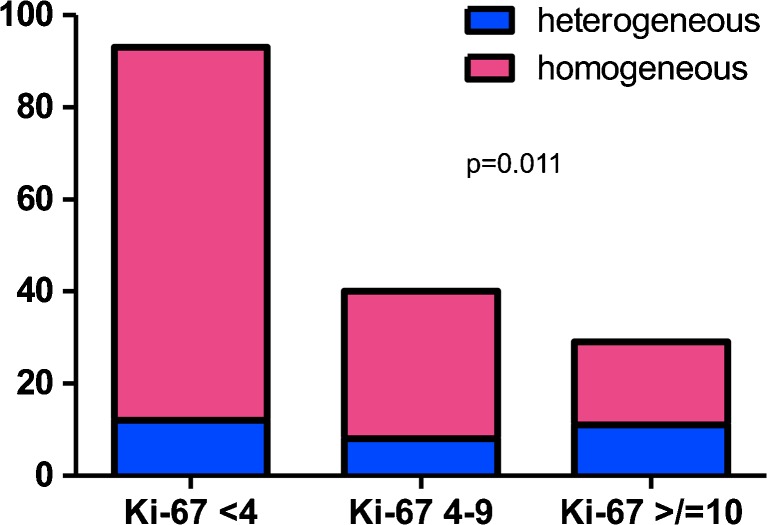
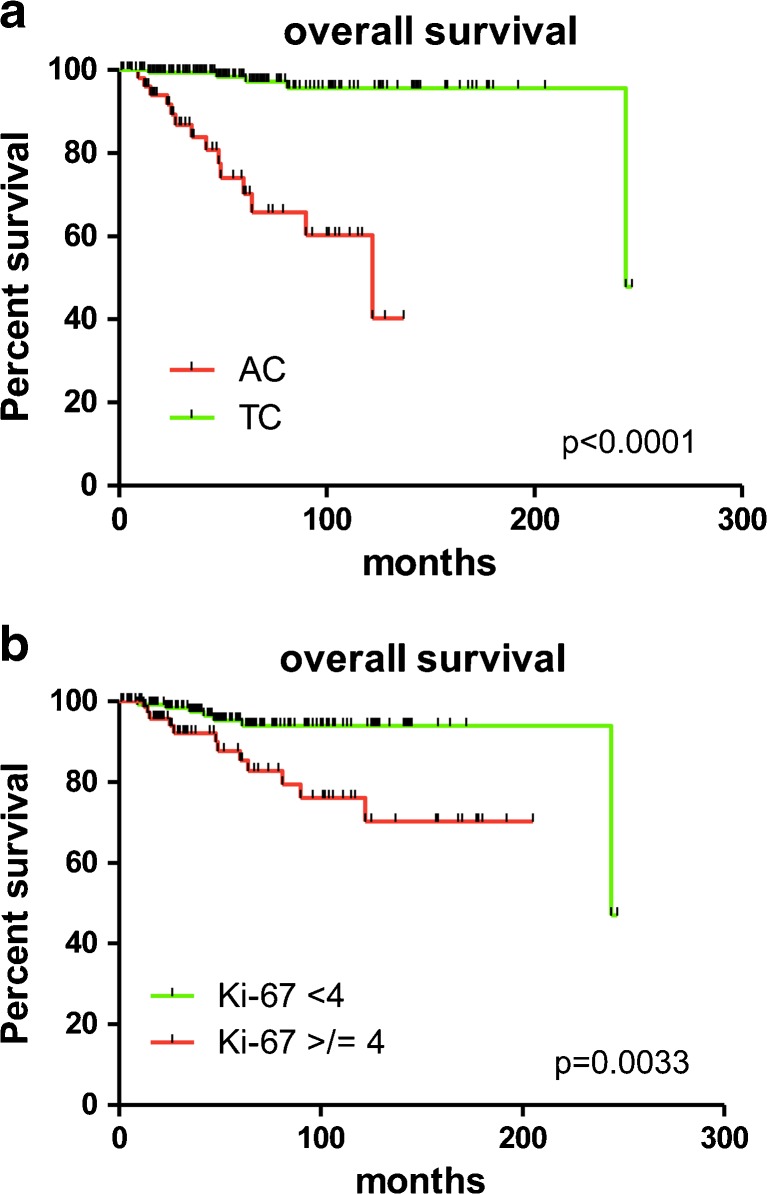
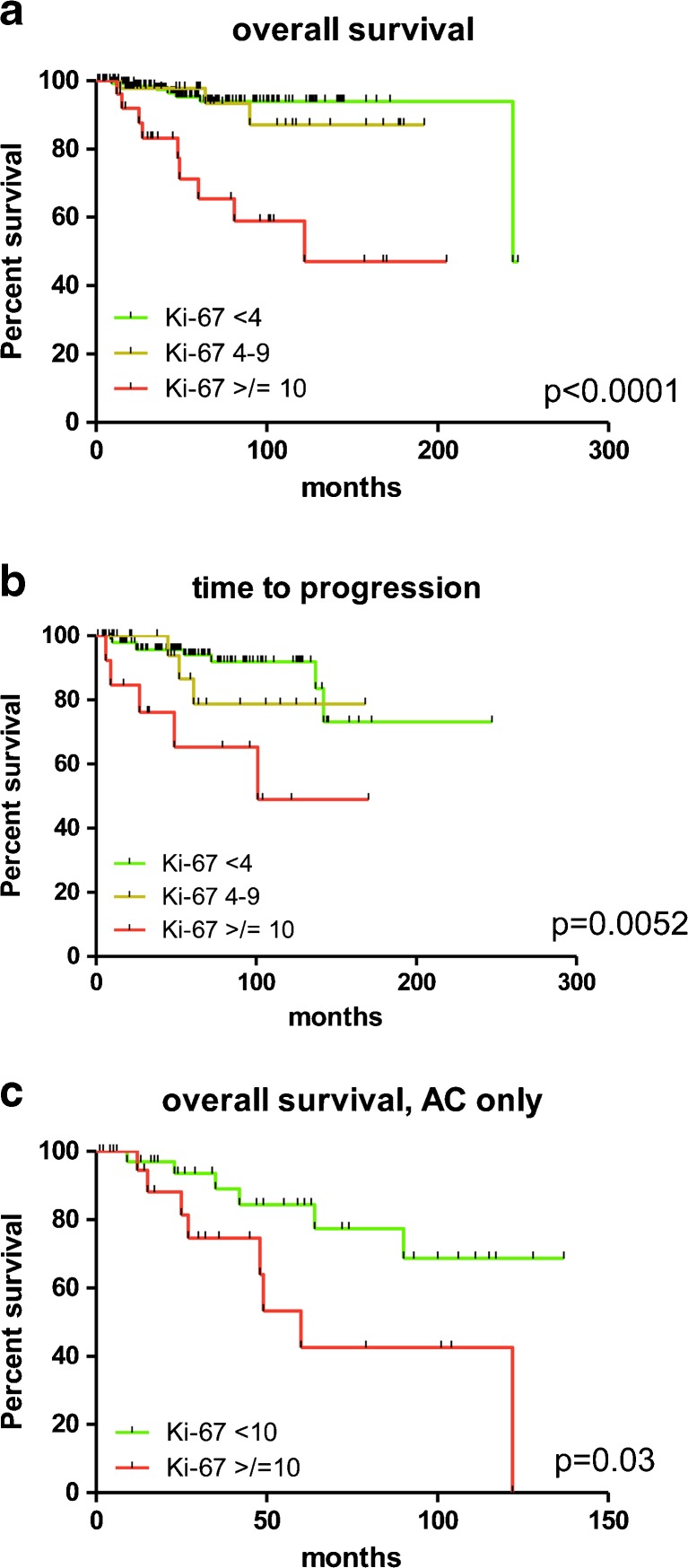
Typical (TCs) and atypical carcinoids (ACs) are defined based on morphological criteria, and no grading system is currently accepted to further stratify these entities. The 2015 WHO classification restricts the Ki-67 role to biopsy or cytology samples, rather than for prognostic prediction. We aimed to investigate whether values and patterns of Ki-67 alone would allow for a clinically meaningful stratification of lung carcinoids, regardless of histological typing. Ki-67 proliferation index and pattern (homogeneous versus heterogeneous expression) were assessed in a cohort of 171 TCs and 68 ACs. Cases were subdivided into three Ki-67 ranges (<4/4-9/≥10%). Correlations with clinicopathological data, univariate and multivariate survival analyses were performed. The majority of cases (61.5%) belonged to the <4% Ki-67 range; 25.1 and 13.4% had a proliferation index of 4-9% and ≥10%, respectively. The <4% Ki-67 subgroup was significantly enriched for TCs (83%, p < 0.0001); ACs were more frequent in the subgroup showing Ki-67 ≥ 10% (75%, p < 0.0001). A heterogeneous Ki-67 pattern was preferentially seen in carcinoids with a Ki-67 ≥10% (38%, p < 0.02). Mean Ki-67 values ≥4 and ≥10% identified categories of poor prognosis both in terms of disease-free and overall survival (p = 0.003 and <0.0001). At multivariate analysis, the two thresholds did not retain statistical significance; however, a Ki-67 ≥ 10% identified a subgroup of dismal prognosis even within ACs (p = 0.03) at univariate analysis. Here, we describe a subgroup of lung carcinoids showing brisk proliferation activity within the necrosis and/or mitotic count-based categories. These patients were associated with specific clinicopathological characteristics, to some extent regardless of histological subtyping.
Keywords: Carcinoid; Heterogeneity; Ki-67; Lung; Prognosis; WHO classification.
Conflict of interest statement
The study has been approved by the local ethical committee (Department of Oncology at San Luigi Hospital, number 17975, October 14th 2015).
The funders (see Acknowledgements) had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors have no potential conflicts of interest to declare.
Figures
References
-
- Travis WD, Brambilla E, Burke A, Marx A, Nicholson A. WHO classification of tumours of the lung, pleura, thymus and heart. 4. Lyon: IARC Press; 2015. - PubMed
-
- Caplin ME, Baudin E, Ferolla P, Filosso P, Garcia-Yuste M, Lim E, Oberg K, Pelosi G, Perren A, Rossi RE, Travis WD, participants Ecc (2015) Pulmonary neuroendocrine (carcinoid) tumors: European neuroendocrine tumor society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann Oncol 26 (8):1604–1620. doi:10.1093/annonc/mdv041 - PubMed
-
- Travis WD (2010) Advances in neuroendocrine lung tumors. Ann Oncol 21 Suppl 7:vii65-71. doi:10.1093/annonc/mdq380 - PubMed
-
- Maurizi G, Ibrahim M, Andreetti C, D'Andrilli A, Ciccone AM, Pomes LM, Menna C, Pellegrini M, Venuta F, Rendina EA. Long-term results after resection of bronchial carcinoid tumour: evaluation of survival and prognostic factors. Interact Cardiovasc Thorac Surg. 2014;19(2):239–244. doi: 10.1093/icvts/ivu109. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
