

Randomized, Noncomparative, Phase II Trial of Early Switch From Docetaxel to Cabazitaxel or Vice Versa, With Integrated Biomarker Analysis, in Men With Chemotherapy-Naïve, Metastatic, Castration-Resistant Prostate Cancer
- PMID: 28632486
- PMCID: PMC5791829
- DOI: 10.1200/JCO.2017.72.4138
Randomized, Noncomparative, Phase II Trial of Early Switch From Docetaxel to Cabazitaxel or Vice Versa, With Integrated Biomarker Analysis, in Men With Chemotherapy-Naïve, Metastatic, Castration-Resistant Prostate Cancer
Abstract
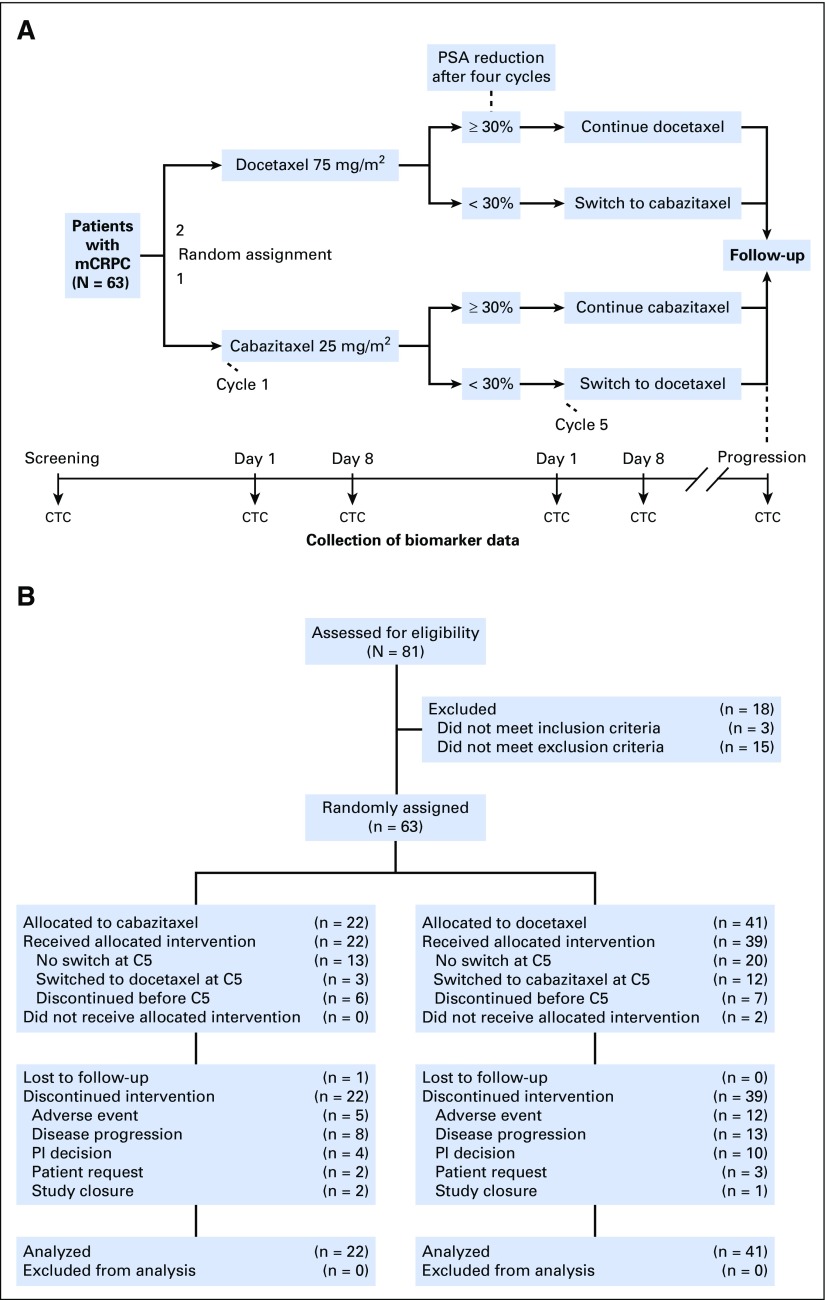
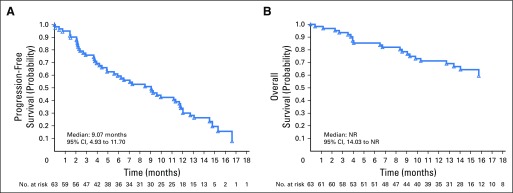
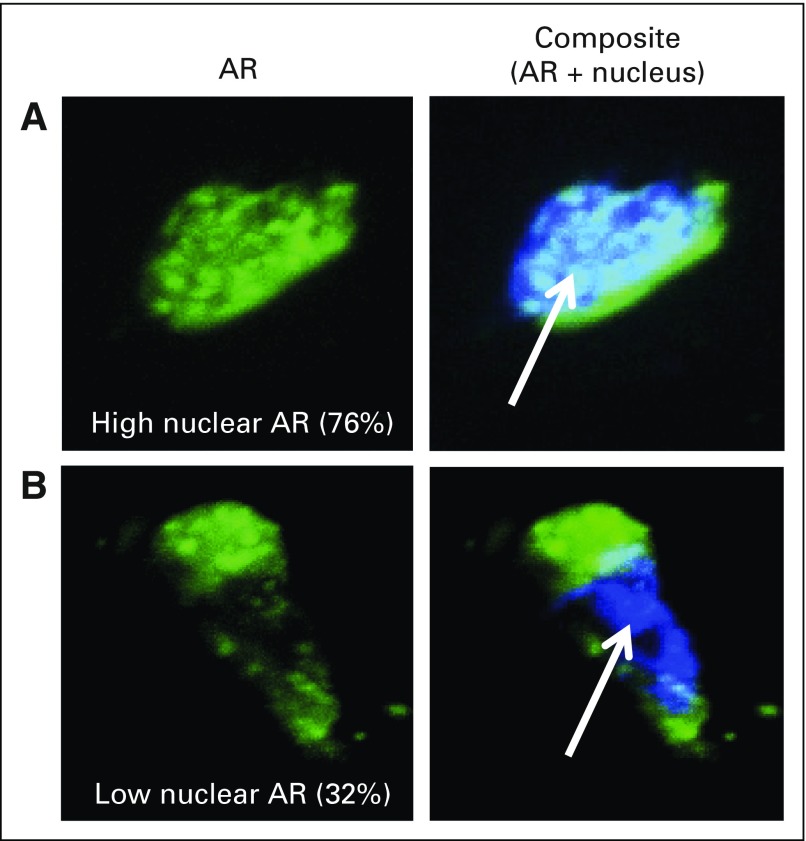
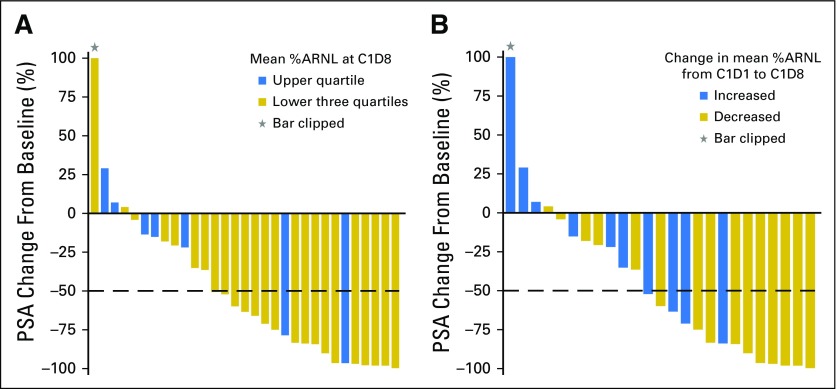
Purpose The TAXYNERGY trial ( ClinicalTrials.gov identifier: NCT01718353) evaluated clinical benefit from early taxane switch and circulating tumor cell (CTC) biomarkers to interrogate mechanisms of sensitivity or resistance to taxanes in men with chemotherapy-naïve, metastatic, castration-resistant prostate cancer. Patients and Methods Patients were randomly assigned 2:1 to docetaxel or cabazitaxel. Men who did not achieve ≥ 30% prostate-specific antigen (PSA) decline by cycle 4 (C4) switched taxane. The primary clinical endpoint was confirmed ≥ 50% PSA decline versus historical control (TAX327). The primary biomarker endpoint was analysis of post-treatment CTCs to confirm the hypothesis that clinical response was associated with taxane drug-target engagement, evidenced by decreased percent androgen receptor nuclear localization (%ARNL) and increased microtubule bundling. Results Sixty-three patients were randomly assigned to docetaxel (n = 41) or cabazitaxel (n = 22); 44.4% received prior potent androgen receptor-targeted therapy. Overall, 35 patients (55.6%) had confirmed ≥ 50% PSA responses, exceeding the historical control rate of 45.4% (TAX327). Of 61 treated patients, 33 (54.1%) had ≥ 30% PSA declines by C4 and did not switch taxane, 15 patients (24.6%) who did not achieve ≥ 30% PSA declines by C4 switched taxane, and 13 patients (21.3%) discontinued therapy before or at C4. Of patients switching taxane, 46.7% subsequently achieved ≥ 50% PSA decrease. In 26 CTC-evaluable patients, taxane-induced decrease in %ARNL (cycle 1 day 1 v cycle 1 day 8) was associated with a higher rate of ≥ 50% PSA decrease at C4 ( P = .009). Median composite progression-free survival was 9.1 months (95% CI, 4.9 to 11.7 months); median overall survival was not reached at 14 months. Common grade 3 or 4 adverse events included fatigue (13.1%) and febrile neutropenia (11.5%). Conclusion The early taxane switch strategy was associated with improved PSA response rates versus TAX327. Taxane-induced shifts in %ARNL may serve as an early biomarker of clinical benefit in patients treated with taxanes.
Figures
Comment in
-
The Who, What, and How of Cabazitaxel Treatment in Metastatic Castration-Resistant Prostate Cancer.J Clin Oncol. 2017 Oct 1;35(28):3175-3177. doi: 10.1200/JCO.2017.74.7931. Epub 2017 Aug 15. J Clin Oncol. 2017. PMID: 28809609 No abstract available.
References
-
- Tannock IF, de Wit R, Berry WR, et al. : Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 351:1502-1512, 2004 - PubMed
-
- de Bono JS, Oudard S, Ozguroglu M, et al. : Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 376:1147-1154, 2010 - PubMed
-
- Jordan MA, Wilson L: Microtubules as a target for anticancer drugs. Nat Rev Cancer 4:253-265, 2004 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
