

Multicenter retrospective study of noncompressible torso hemorrhage: Anatomic locations of bleeding and comparison of endovascular versus open approach
- PMID: 28632581
- PMCID: PMC5484539
- DOI: 10.1097/TA.0000000000001530
Multicenter retrospective study of noncompressible torso hemorrhage: Anatomic locations of bleeding and comparison of endovascular versus open approach
Abstract
Background: Rational development of technology for rapid control of noncompressible torso hemorrhage (NCTH) requires detailed understanding of what is bleeding. Our objectives were to describe the anatomic location of truncal bleeding in patients presenting with NCTH and compare endovascular (ENDO) management versus open (OPEN) management.
Methods: This is a retrospective study of adult trauma patients with NCTH admitted to four urban Level I trauma centers in the Houston and San Antonio metropolitan areas in 2008 to 2012. Inclusion criteria include named axial torso vessel disruption, Abbreviated Injury Scale chest or abdomen score of 3 or higher with shock (base excess, <-4) or truncal operation in 90 minutes or less, or pelvic fracture with ring disruption. Exclusion criteria include isolated hip fractures, falls from standing, or prehospital cardiopulmonary resuscitation. After dichotomizing into OPEN, ENDO, and resuscitative thoracotomy (RT) groups based on the initial approach to control NCTH, a mixed-effects Poisson regression with robust error variance (controlling for age, mechanism, Injury Severity Score, shock, hypotension, and severe head injury as fixed effects and site as a random effect) was used to test the hypothesis that ENDO was associated with reduced in-hospital mortality in NCTH patients.
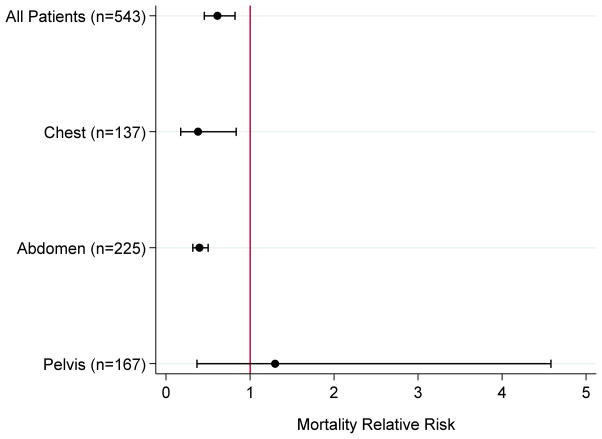
Results: Five hundred forty-three patients with NCTH underwent ENDO (n = 166, 31%), OPEN (n = 309, 57%), or RT (n = 68, 12%). Anatomic bleeding locations were 25% chest, 41% abdomen, and 31% pelvis. ENDO was used to treat relatively few types of vascular injuries, whereas OPEN and RT injuries were more diverse. ENDO patients had more blunt trauma (95% vs. 34% vs. 32%); severe injuries (median Injury Severity Score, 34 vs. 27 vs. 21), and increased time to intervention (median, 298 vs. 92 vs. 51 minutes) compared with OPEN and RT. Mortality was 15% versus 20% versus 79%. ENDO was associated with decreased mortality compared to OPEN (relative risk, 0.58; 95% confidence interval, 0.46-0.73).
Conclusion: Although ENDO may reduce mortality in NCTH patients, significant group differences limit the generalizability of this finding.
Level of evidence: Therapeutic, level V.
Conflict of interest statement
Figures
References
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38(2):185–93. - PubMed
-
- Tien HC, Spencer F, Tremblay LN, Rizoli SB, Brenneman FD. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma. 2007;62(1):142–6. - PubMed
-
- Kotwal RS, Montgomery HR, Kotwal BM, Champion HR, Butler FK, Jr, Mabry RL, Cain JS, Blackbourne LH, Mechler KK, Holcomb JB. Eliminating Preventable Death on the Battlefield. Arch Surg. 2011;146(12):1350–8. - PubMed
-
- Holcomb JB, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, Alarcon LH, Bai Y, Brasel KJ, Bulger EM, et al. PROMMTT Study Group. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013;148:127–36. - PMC - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. PROPPR study group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313:471–82. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
