

Clinical features and treatment outcomes in large granular lymphocytic leukemia (LGLL)
- PMID: 28633612
- PMCID: PMC8694069
- DOI: 10.1080/10428194.2017.1339880
Clinical features and treatment outcomes in large granular lymphocytic leukemia (LGLL)
Abstract
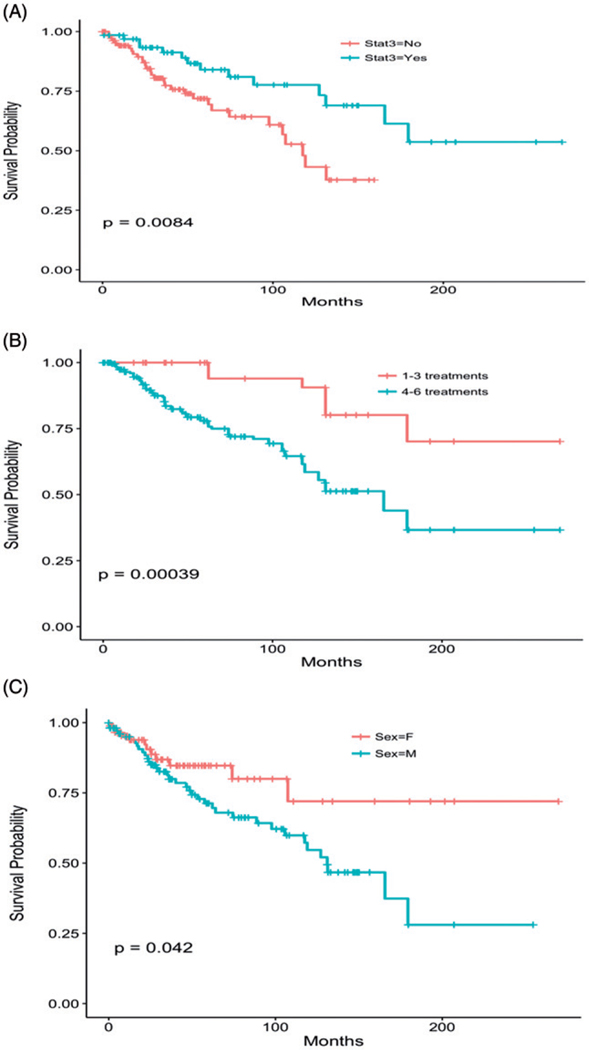
Large granular lymphocytic leukemia (LGLL) represents a clonal/oligoclonal lymphoproliferation of cytotoxic T and natural killer cells often associated with STAT3 mutations. When symptomatic, due to mostly anemia and neutropenia, therapy choices are often empirically-based, because only few clinical trials and systematic studies have been performed. Incorporating new molecular and flow cytometry parameters, we identified 204 patients fulfilling uniform criteria for LGLL diagnoses and analyzed clinical course with median follow-up of 36 months, including responses to treatments. While selection of initial treatment was dictated by clinical features, the initial responses, as well as overall responses to methotrexate (MTX), cyclosporine (CsA), and cyclophosphamide (CTX), were similar at 40-50% across drugs. Sequential use of these drugs resulted in responses in most cases: only 10-20% required salvage therapies such as ATG, Campath, tofacitinib, splenectomy or abatacept. MTX yielded the most durable responses. STAT3-mutated patients required therapy more frequently and had better overall survival.
Keywords: NK-LGLL; STAT3 mutation; T-LGLL.
Conflict of interest statement
Figures
References
-
- Loughran TP Jr, Kadin ME, Starkebaum G, et al. Leukemia of large granular lymphocytes: association with clonal chromosomal abnormalities and autoimmune neutropenia, thrombocytopenia and hemolytic anemia. Ann Intern Med. 1985;102:169–175. - PubMed
-
- Loughran TP Jr. Clonal diseases of large granular lymphocytes. Blood. 1993;82:1–14. - PubMed
-
- Epling-Burnette PK, Loughran TP Jr. Survival signals in leukemic large granular lymphocytes. Semin Hematol. 2003;40:213–220. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous