

Influence of the number and timing of malaria episodes during pregnancy on prematurity and small-for-gestational-age in an area of low transmission
- PMID: 28633672
- PMCID: PMC5479010
- DOI: 10.1186/s12916-017-0877-6
Influence of the number and timing of malaria episodes during pregnancy on prematurity and small-for-gestational-age in an area of low transmission
Abstract
Background: Most evidence on the association between malaria in pregnancy and adverse pregnancy outcomes focuses on falciparum malaria detected at birth. We assessed the association between the number and timing of falciparum and vivax malaria episodes during pregnancy on small-for-gestational-age (SGA) and preterm birth.
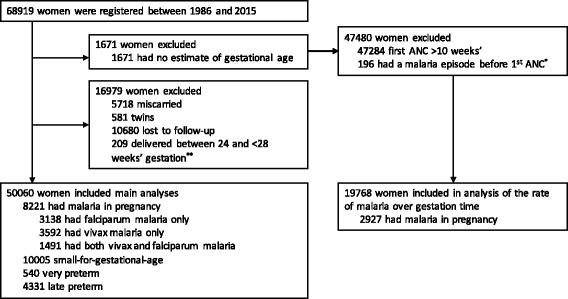
Methods: We analysed observational data collected from antenatal clinics on the Thailand-Myanmar border (1986-2015). We assessed the effects of the total number of malaria episodes in pregnancy on SGA and the effects of malaria in pregnancy on SGA, very preterm birth, and late preterm birth, by the gestational age at malaria detection and treatment using logistic regression models with time-dependent malaria variables (monthly intervals). World Health Organisation definitions of very preterm birth (≥28 and <32 weeks) and late preterm birth (≥32 and <37 weeks) and international SGA standards were used.
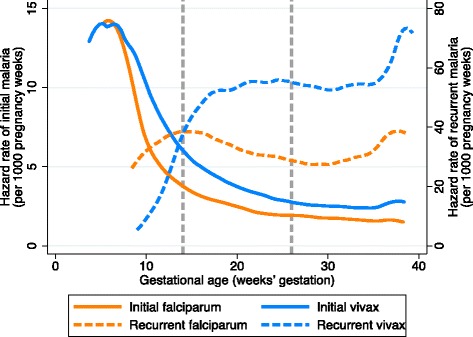
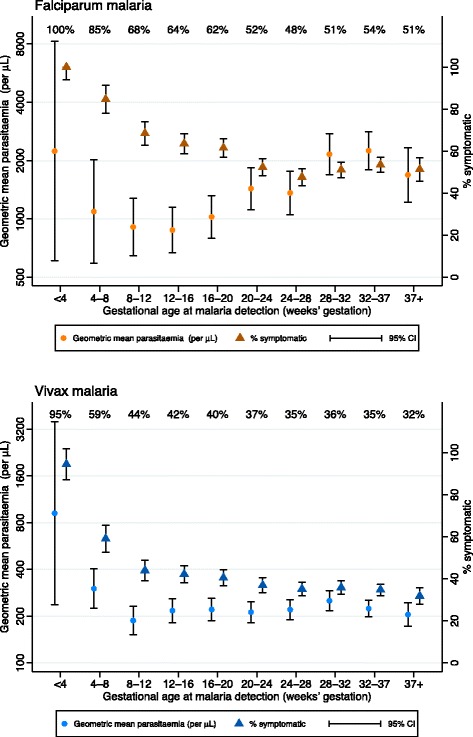
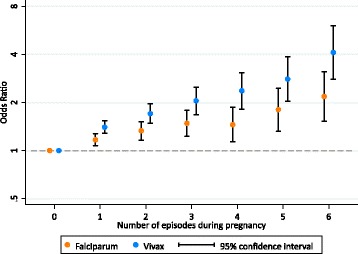
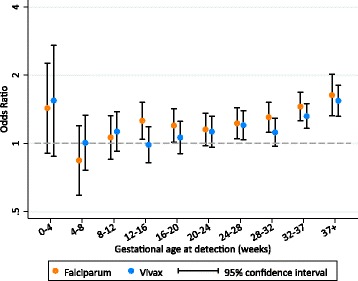
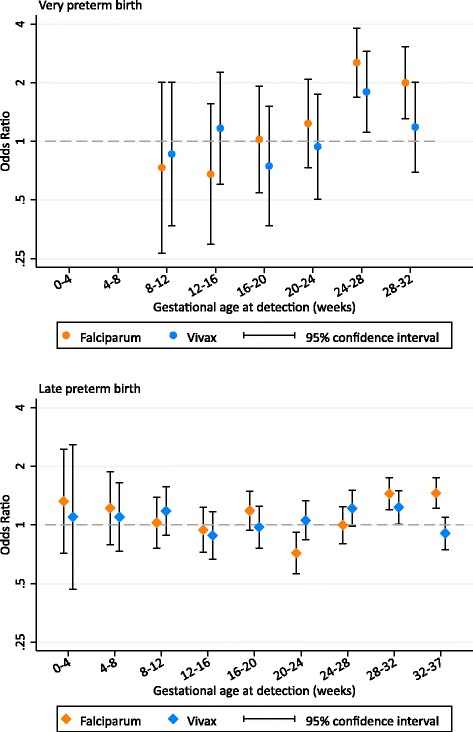
Results: Of 50,060 pregnant women followed, 8221 (16%) had malaria during their pregnancy. Of the 50,060 newborns, 10,005 (21%) were SGA, 540 (1%) were very preterm, and 4331 (9%) were late preterm. The rates of falciparum and vivax malaria were highest at 6 and 5 weeks' gestation, respectively. The odds of SGA increased linearly by 1.13-fold (95% confidence interval: 1.09, 1.17) and 1.27-fold (1.21, 1.33) per episode of falciparum and vivax malaria, respectively. Falciparum malaria at any gestation period after 12-16 weeks and vivax malaria after 20-24 weeks were associated with SGA (falciparum odds ratio, OR range: 1.15-1.63 [p range: <0.001-0.094]; vivax OR range: 1.12-1.54 [p range: <0.001-0.138]). Falciparum malaria at any gestation period after 24-28 weeks was associated with either very or late preterm birth (OR range: 1.44-2.53; p range: <0.001-0.001). Vivax malaria at 24-28 weeks was associated with very preterm birth (OR: 1.79 [1.11, 2.90]), and vivax malaria at 28-32 weeks was associated with late preterm birth (OR: 1.23 [1.01, 1.50]). Many of these associations held for asymptomatic malaria.
Conclusions: Protection against malaria should be started as early as possible in pregnancy. Malaria control and elimination efforts in the general population can avert the adverse consequences associated with treated asymptomatic malaria in pregnancy.
Keywords: Gestation; Malaria in pregnancy; Preterm birth; Small-for-gestational-age; Timing.
Figures
References
-
- Matangila JR, Lufuluabo J, Ibalanky AL, da Luz RA I, Lutumba P, Van Geertruyden J-P. Asymptomatic Plasmodium falciparum infection is associated with anaemia in pregnancy and can be more cost-effectively detected by rapid diagnostic test than by microscopy in Kinshasa, Democratic Republic of the Congo. Malar J. 2014;13:132. doi: 10.1186/1475-2875-13-132. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
