

Different levels of blood pressure, different benefit from dual antiplatelet therapy in minor stroke or TIA patients
- PMID: 28634365
- PMCID: PMC5478626
- DOI: 10.1038/s41598-017-04169-8
Different levels of blood pressure, different benefit from dual antiplatelet therapy in minor stroke or TIA patients
Abstract
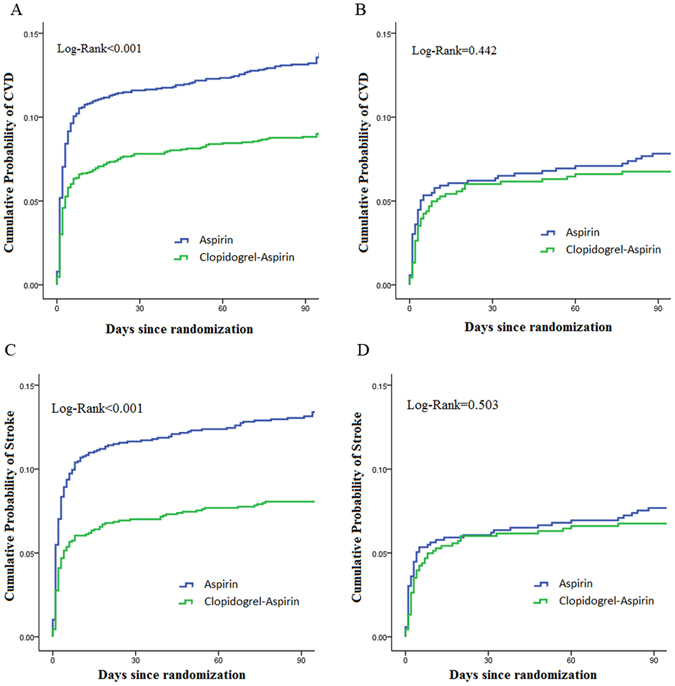
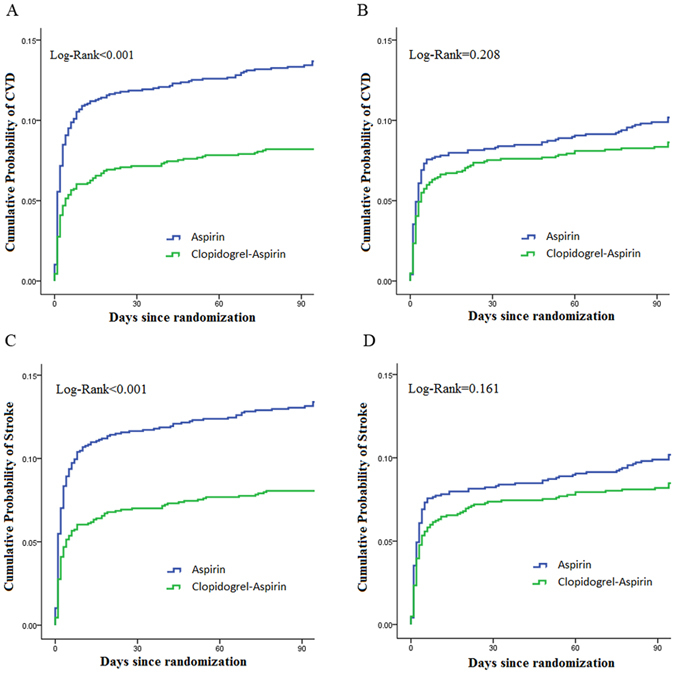
The study aimed to evaluate whether the benefits of dual antiplatelet therapy would be influenced by blood pressure (BP) levels, among acute minor stroke or transient ischemic attack (TIA). In CHANCE (Clopidogrel in High-Risk Patients with Acute Nondisabling cerebrovascular Events) trail, Patients were stratified by systolic BP (SBP) and diastolic BP (DBP) level measured on admission, respectively, using the supine position BP within 24 hours after symptoms onset. The primary efficacy outcome was stroke recurrence, bleeding was the safety outcome. Patients with SBP ≥ 140 mmHg, dual antiplatelet treatment could reduce the risk of stroke recurrence significantly (HR 0.654, 95% CI 0.529-0.793, p < 0.001) than mono antiplatelet therapy. And patients with DBP ≥ 90 mmHg, clopidogrel-aspirin significantly reduced the risk of recurrent stroke (HR 0.588, 95% CI 0.463-0.746, p < 0.001), compared with aspirin alone. However, in patients with SBP < 140 mmHg or DBP < 90 mmHg, no significant difference was observed between clopidogrel plus aspirin and aspirin alone. there was no difference in bleeding episodes by treatment assignment across categories of SBP or DBP. Patients with SBP ≥ 140 mmHg or DBP ≥ 90 mmHg after minor stroke or TIA got more benefits from dual antiplatelet therapy. Bleeding risk from dual antiplatelet treatment did not increase among patients with higher BP level on admission.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
