

Cystic lesions of peripheral nerves: Are we missing the diagnosis of the intraneural ganglion cyst?
- PMID: 28634514
- PMCID: PMC5441458
- DOI: 10.4329/wjr.v9.i5.230
Cystic lesions of peripheral nerves: Are we missing the diagnosis of the intraneural ganglion cyst?
Abstract
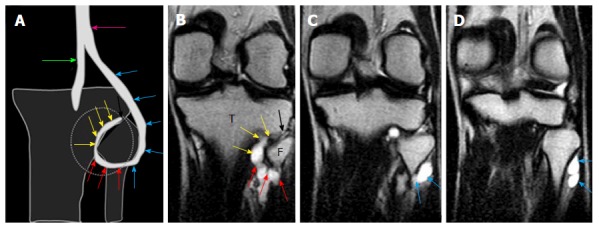
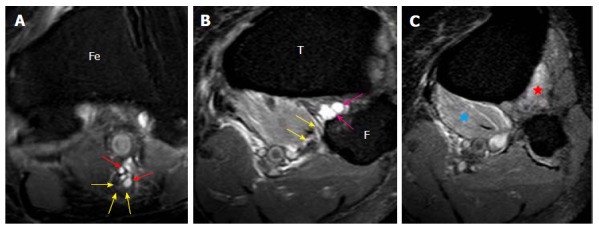
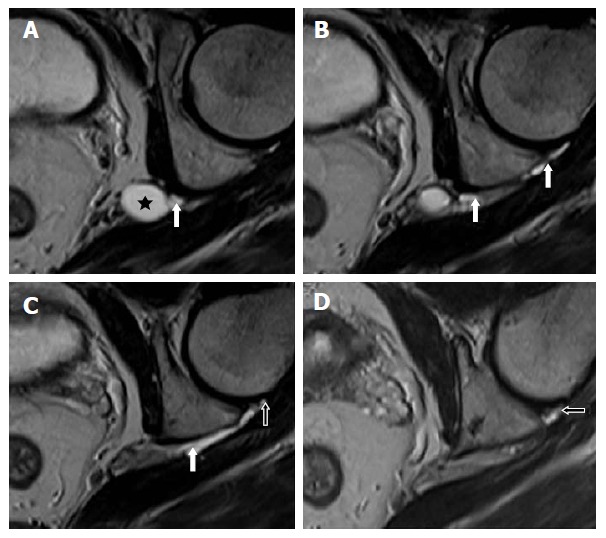
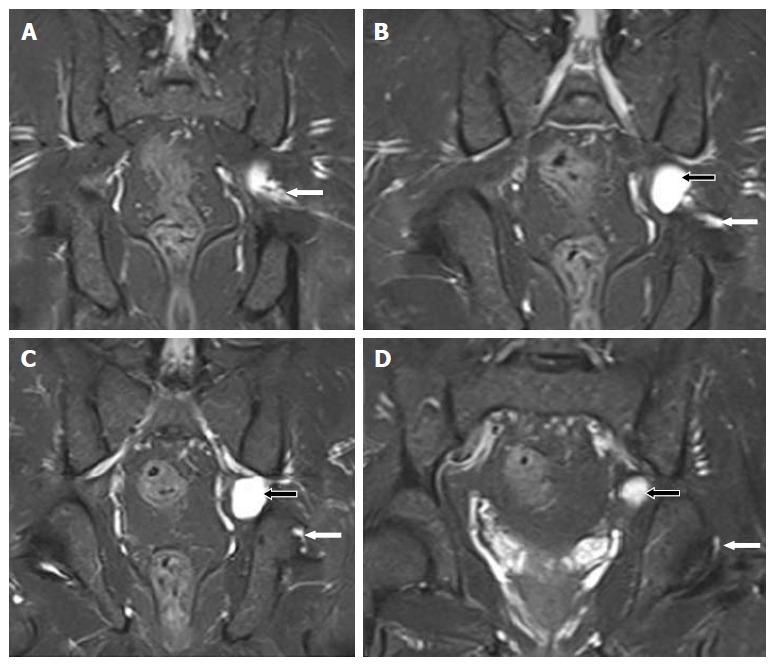
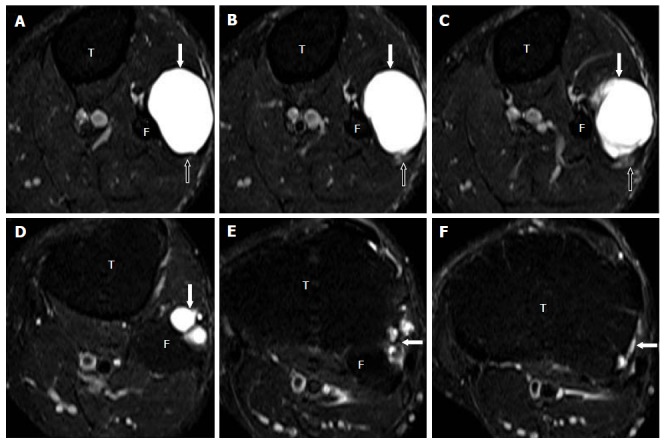
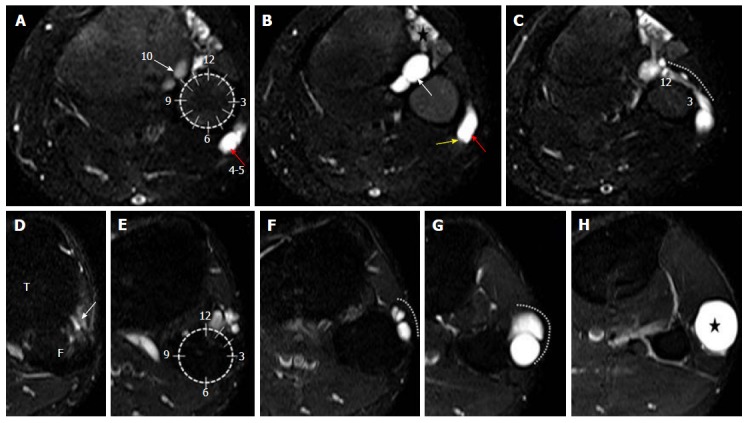
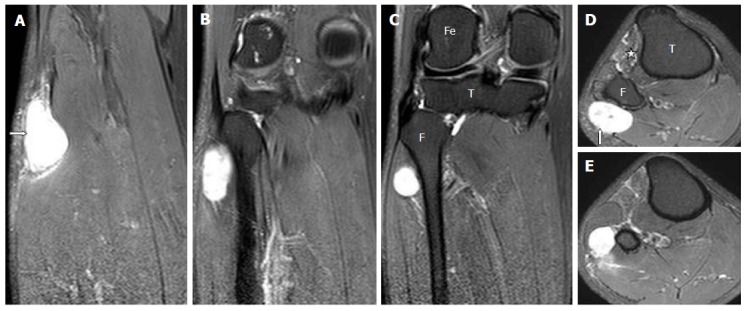
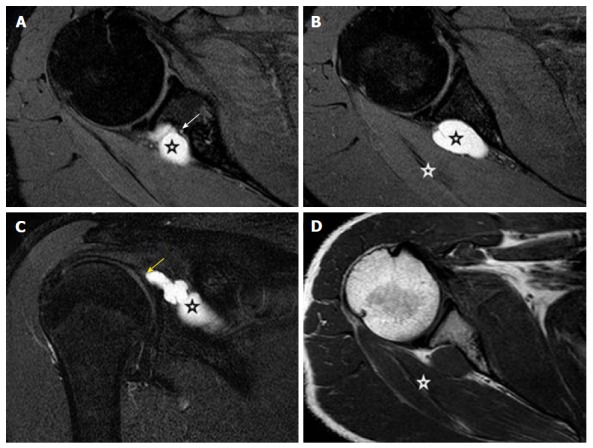
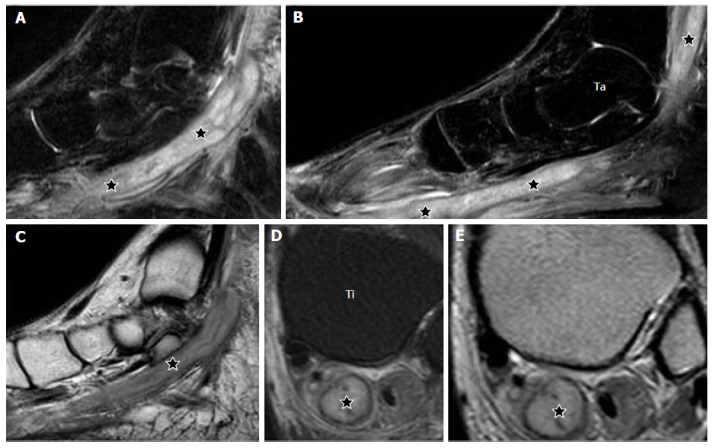
Aim: To highlight the salient magnetic resonance imaging (MRI) features of the intraneural ganglion cyst (INGC) of various peripheral nerves for their precise diagnosis and to differentiate them from other intra and extra-neural cystic lesions.
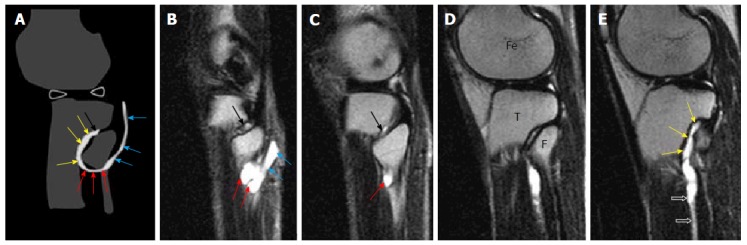
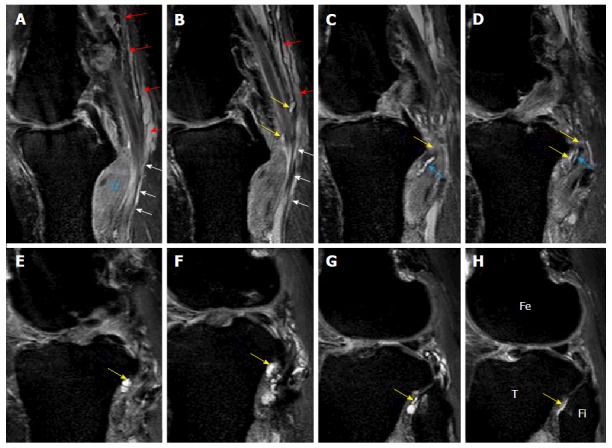
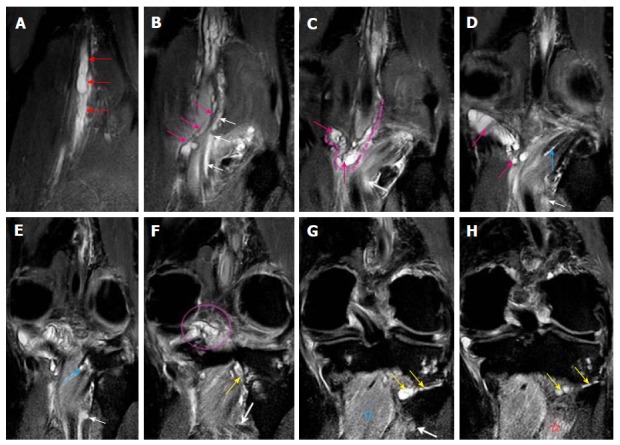
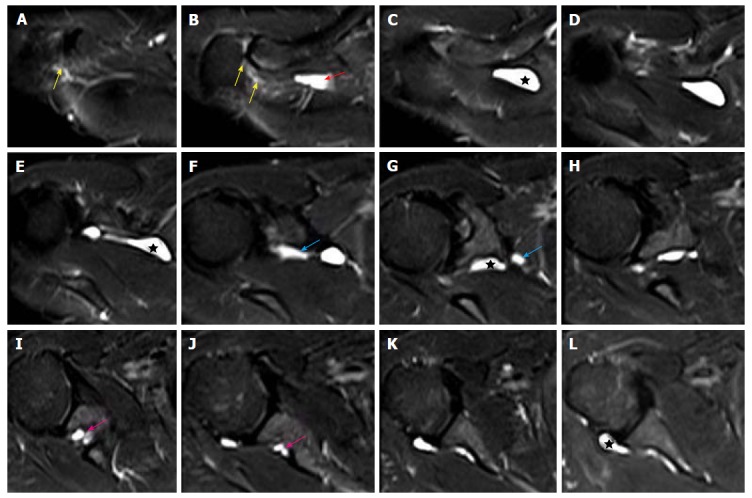
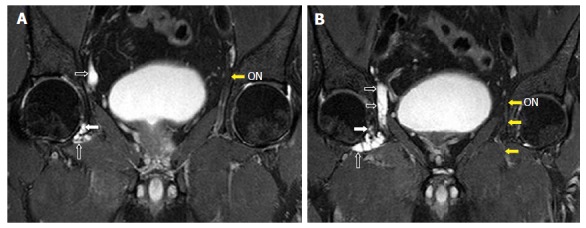
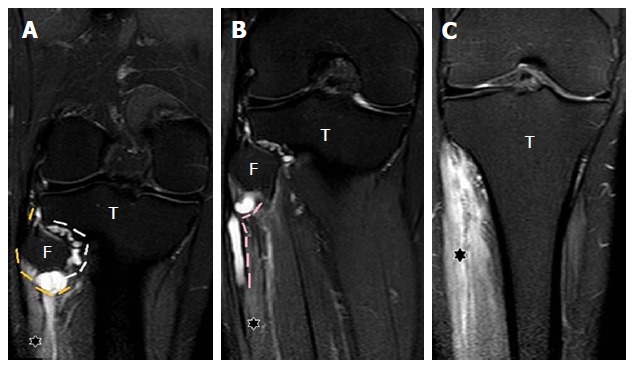
Methods: A retrospective analysis of the magnetic resonance (MR) images of a cohort of 245 patients presenting with nerve palsy involving different peripheral nerves was done. MR images were analyzed for the presence of a nerve lesion, and if found, it was further characterized as solid or cystic. The serial axial, coronal and sagittal MR images of the lesions diagnosed as INGC were studied for their pattern and the anatomical extent along the course of the affected nerve and its branches. Its relation to identifiable anatomical landmarks, intra-articular communication and presence of denervation changes in the muscles supplied by involved nerve was also studied.
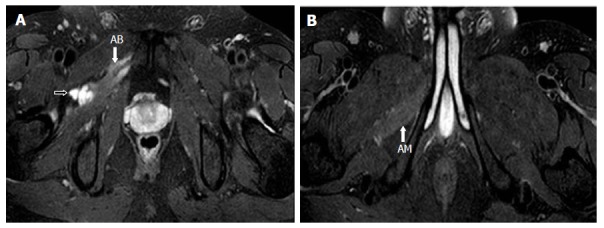
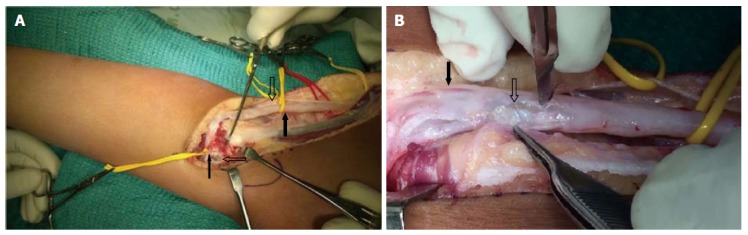
Results: A total of 45 cystic lesions in the intra or extraneural locations of the nerves were identified from the 245 MR scans done for patients presenting with nerve palsy. Out of these 45 cystic lesions, 13 were diagnosed to have INGC of a peripheral nerve on MRI. The other cystic lesions included extraneural ganglion cyst, paralabral cyst impinging upon the suprascapular nerve, cystic schwannoma and nerve abscesses related to Hansen's disease involving various peripheral nerves. Thirteen lesions of INGC were identified in 12 patients. Seven of these affected the common peroneal nerve with one patient having a bilateral involvement. Two lesions each were noted in the tibial and suprascapular nerves, and one each in the obturator and proximal sciatic nerve. An intra-articular connection along the articular branch was demonstrated in 12 out of 13 lesions. Varying stages of denervation atrophy of the supplied muscles of the affected nerves were seen in 7 cases. Out of these 13 lesions in 12 patients, 6 underwent surgery.
Conclusion: INGC is an important cause of reversible mono-neuropathy if diagnosed early and surgically treated. Its classic MRI pattern differentiates it from other lesions of the peripheral nerve and aid in its therapeutic planning. In each case, the joint connection has to be identified preoperatively, and the same should be excised during surgery to prevent further cyst recurrence.
Keywords: Extra-neural; Ganglion cyst; Intra-neural; Magnetic resonance imaging; Peripheral nerves.
Conflict of interest statement
Conflict-of-interest statement: There are no conflicts of interest to report.
Figures
References
-
- van Brakel WH, Nicholls PG, Das L, Barkataki P, Suneetha SK, Jadhav RS, Maddali P, Lockwood DN, Wilder-Smith E, Desikan KV. The INFIR Cohort Study: investigating prediction, detection and pathogenesis of neuropathy and reactions in leprosy. Methods and baseline results of a cohort of multibacillary leprosy patients in north India. Lepr Rev. 2005;76:14–34. - PubMed
-
- de Freitas MR, Nascimento OJ, Quaglino EA, Oliveira A, Hahn MD. Small-fiber polyneuropathy in leprosy without skin changes: study of 17 cases. Arq Neuropsiquiatr. 2003;61:542–546. - PubMed
-
- World Health Organization, Global leprosy situation, Relevé Épidémiologique Hebd. Sect. Hygiène Secrétariat Société Nations Wkly Epidemiol Rec Health Sect Secr Leag Nation 2005; 80: 289-295 - PubMed
-
- Joyce M, Scollard D. 2004. Lepr. Hansens Dis. Conns Curr. Ther., edition 1, Saunders, Philadelphia; pp. 100–105.
LinkOut - more resources
Full Text Sources
Other Literature Sources
