

Categorical Risk Perception Drives Variability in Antibiotic Prescribing in the Emergency Department: A Mixed Methods Observational Study
- PMID: 28634909
- PMCID: PMC5602760
- DOI: 10.1007/s11606-017-4099-6
Categorical Risk Perception Drives Variability in Antibiotic Prescribing in the Emergency Department: A Mixed Methods Observational Study
Abstract
Background: Adherence to evidence-based antibiotic therapy guidelines for treatment of upper respiratory tract infections (URIs) varies widely among clinicians. Understanding this variability is key for reducing inappropriate prescribing.
Objective: To measure how emergency department (ED) clinicians' perceptions of antibiotic prescribing risks affect their decision-making.
Design: Clinician survey based on fuzzy-trace theory, a theory of medical decision-making, combined with retrospective data on prescribing outcomes for URI/pneumonia visits in two EDs. The survey predicts the categorical meanings, or gists, that individuals derive from given information.
Participants: ED physicians, residents, and physician assistants (PAs) who completed surveys and treated patients with URI/pneumonia diagnoses between August 2014 and December 2015.
Main measures: Gists derived from survey responses and their association with rates of antibiotic prescribing per visit.
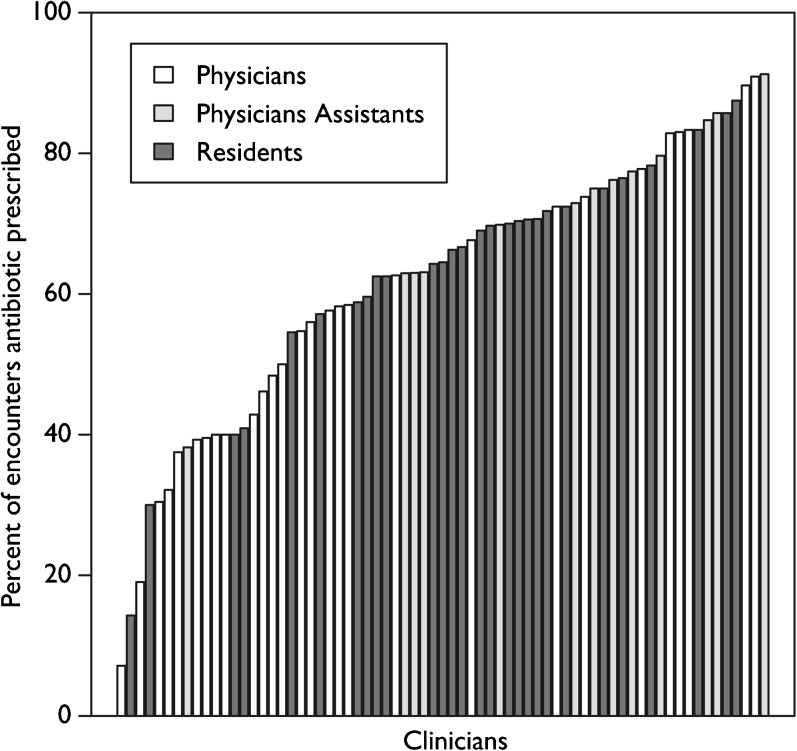
Key results: Of 4474 URI/pneumonia visits, 2874 (64.2%) had an antibiotic prescription. However, prescribing rates varied from 7% to 91% for the 69 clinicians surveyed (65.2% response rate). Clinicians who framed therapy-prescribing decisions as a categorical choice between continued illness and possibly beneficial treatment ("why not take a risk?" gist, which assumes antibiotic therapy is essentially harmless) had higher rates of prescribing (OR 1.28 [95% CI, 1.06-1.54]). Greater agreement with the "antibiotics may be harmful" gist was associated with lower prescribing rates (OR 0.81 [95% CI, 0.67-0.98]).
Conclusions: Our results indicate that clinicians who perceive prescribing as a categorical choice between patients remaining ill or possibly improving from therapy are more likely to prescribe antibiotics. However, this strategy assumes that antibiotics are essentially harmless. Clinicians who framed decision-making as a choice between potential harms from therapy and continued patient illness (e.g., increased appreciation of potential harms) had lower prescribing rates. These results suggest that interventions to reduce inappropriate prescribing should emphasize the non-negligible possibility of serious side effects.
Keywords: antibiotic resistance; drivers of decision-making; fuzzy-trace theory; gist of antibiotic therapy; non-negligible risks of unnecessary antibiotics.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Capsule Commentary on Klein et al., Categorical Risk Perception Drives Variability in Antibiotic Prescribing in the Emergency Department: a Mixed Methods Observational Study.J Gen Intern Med. 2017 Oct;32(10):1130. doi: 10.1007/s11606-017-4136-5. J Gen Intern Med. 2017. PMID: 28752357 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
