

Efficacy and safety of ultrasound-guided implantation of fiducial markers in the liver for stereotactic body radiation therapy
- PMID: 28636658
- PMCID: PMC5479553
- DOI: 10.1371/journal.pone.0179676
Efficacy and safety of ultrasound-guided implantation of fiducial markers in the liver for stereotactic body radiation therapy
Abstract
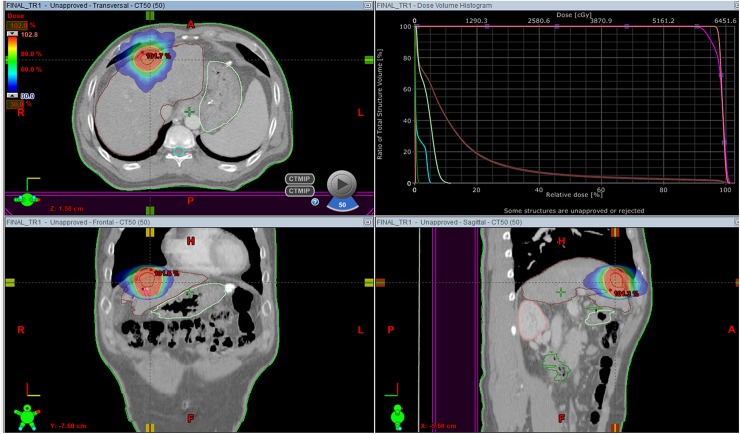
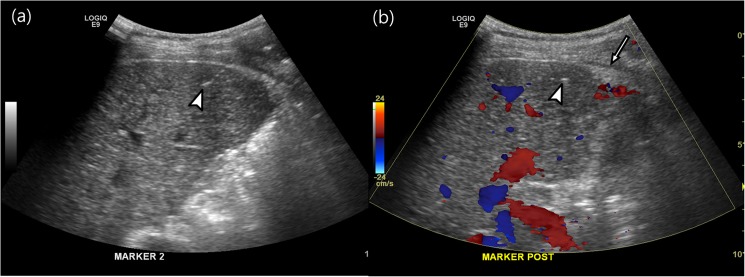
Objective: Stereotactic body radiation therapy (SBRT) for the treatment of a malignancy in the liver requires the perilesional implantation of fiducial markers for lesion detection. The purpose of this study is to evaluate the efficacy and safety of ultrasound (US) -guided marker implantation for SBRT.
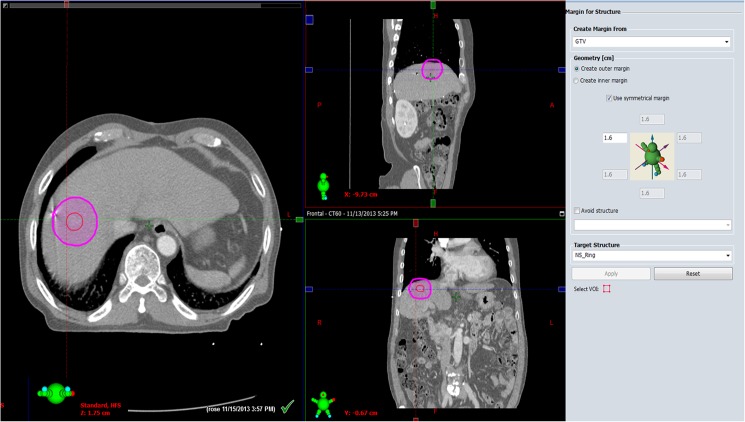
Methods: We retrospectively reviewed 299, US-guided, intrahepatic fiducial markers implanted in 101 patients between November 2013 and September 2014. SBRT-planning CT images were analyzed to determine the technical success of the implantation, the mean distance between the tumor margin and the marker, with the ideal location of fiducials defined as the distance between a marker and a tumor less than 3 cm and the distance between markers greater than 2 cm according to the tumor conspicuity seen on gray-scale US and the artifact obscuring tumor margins. We also evaluated procedure-related major and minor complications.
Results: Technical success was achieved in 291 (97.3%) fiducial marker implantations. The mean distance between the tumor and the marker was 3.1 cm (S.D., 2.1 cm; range, 0-9.5 cm). Of 101 patients, 72 lesions (71.3%, 2.2 ± 1.0 cm; range, 0-3.0 cm) had fiducial markers located in an ideal location. The ideal location of fiducials was more common in visible lesions than in poorly conspicuous lesions (90.2% vs. 52.0%, P < 0.001). Seventeen markers (5.8%) developed beam-hardening artifacts obscuring the tumor margins. There were no major complications, although 12 patients (11.9%) developed minor complications.
Conclusions: US-guided implantation of fiducial markers in the liver is an effective and safe procedure with only rare complications.
Conflict of interest statement
Figures

References
-
- Das IJ, Downes MB, Corn BW, Curran WJ, Werner-Wasik M, Andrews DW. Characteristics of a dedicated linear accelerator-based stereotactic radiosurgery-radiotherapy unit. Radiother Oncol. 1996; 38: 61–68. - PubMed
-
- Oldrini G, Taste-George H, Renard-Oldrini S, Baumann AS, Marchesi V, Troufleau P, et al. Implantation of fiducial markers in the liver for stereotactic body radiation therapy: Feasibility and results. Diagn Interv Imaging. 2014; 96: 589–592. doi: 10.1016/j.diii.2014.01.010 - DOI - PubMed
-
- Facciuto ME, Singh MK, Rochon C, Sharma J, Gimenez C, Katta U, et al. Stereotactic body radiation therapy in hepatocellular carcinoma and cirrhosis: evaluation of radiological and pathological response. J Surg Oncol. 2012; 105: 692–698. doi: 10.1002/jso.22104 - DOI - PubMed
-
- Yoon SM, Lim Y-S, Park MJ, Kim SY, Cho B, Shim JH, et al. Stereotactic body radiation therapy as an alternative treatment for small hepatocellular carcinoma. PLoS One. 2013; 8: e79854 doi: 10.1371/journal.pone.0079854 - DOI - PMC - PubMed
-
- Dawson LA, McGinn CJ, Normolle D, Ten Haken RK, Walker S, Ensminger W, et al. Escalated focal liver radiation and concurrent hepatic artery fluorodeoxyuridine for unresectable intrahepatic malignancies. Journal of Clinical Oncology. 2000; 18: 2210–2218. doi: 10.1200/JCO.2000.18.11.2210 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
