

doi: 10.1001/jamasurg.2017.1586.
Practice- vs Physician-Level Variation in Use of Active Surveillance for Men With Low-Risk Prostate Cancer: Implications for Collaborative Quality Improvement
Affiliations
- PMID: 28636713
- PMCID: PMC5831460
- DOI: 10.1001/jamasurg.2017.1586
Item in Clipboard
Practice- vs Physician-Level Variation in Use of Active Surveillance for Men With Low-Risk Prostate Cancer: Implications for Collaborative Quality Improvement
JAMA Surg.
.
Abstract
This study examines the proportion of men treated primarily with active surveillance across practices and among urologists in the Michigan Urological Surgery Improvement Collaborative.
Conflict of interest statement
Figures
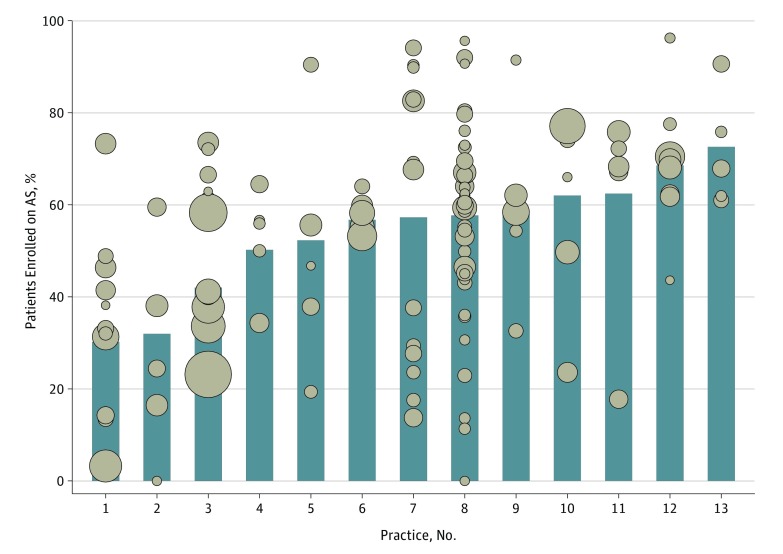
Median patient age was 64 years; median prostate-specific antigen level was 5.0 ng/mL; and Charlson comorbidity score was 0 for 1868 men, 1 for 415 men, and 2 or higher for 360 men. Adjusted AS rates for each urologist and practice were estimated using a multivariable logistic regression model fit to account for differences in patient age and comorbidity among urologists. In the model, age was a continuous predictor, and Charlson comorbidity was a categorical predictor (categories = 0, 1, and ≥2). We defined low-risk according to criteria from the National Comprehensive Cancer Network (ie, clinical stage ≤T2a, prostate-specific antigen <10 ng/mL, and biopsy Gleason score ≤6). The number of urologists per practice varies from 5 to 38. The size of each dot is scaled to represent individual clinician panel size (range, 5-141).
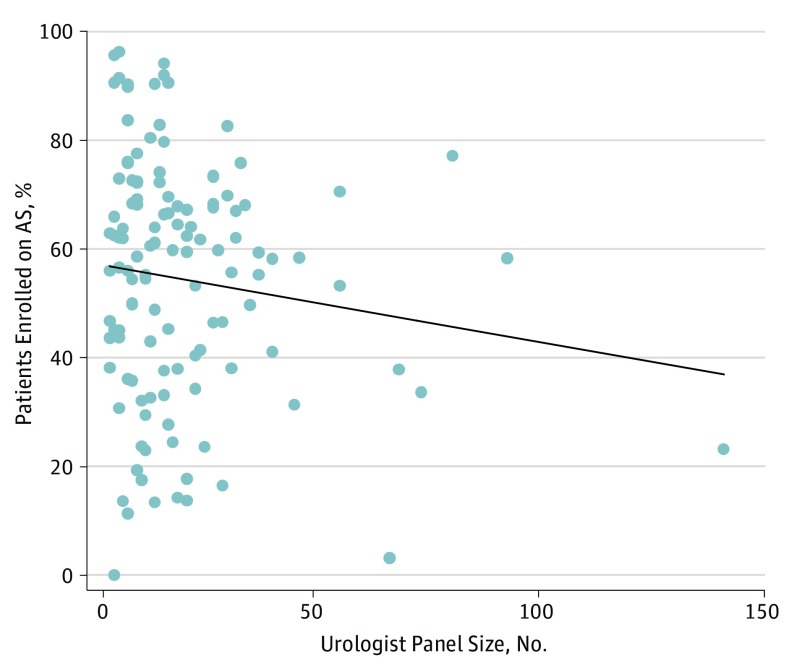
aUrologist panel size = number of men with National Comprehensive Cancer Network low-risk prostate cancer a given urologist primarily treated.
References
-
- Cooperberg MR, Carroll PR. Trends in management for patients with localized prostate cancer, 1990-2013. JAMA. 2015;314(1):80-82. - PubMed
-
- Womble PR, Montie JE, Ye Z, Linsell SM, Lane BR, Miller DC; Michigan Urological Surgery Improvement Collaborative . Contemporary use of initial active surveillance among men in Michigan with low-risk prostate cancer. Eur Urol. 2015;67(1):44-50. - PubMed
-
- Cher ML, Dhir A, Auffenberg GB, et al. ; Michigan Urological Surgery Improvement Collaborative . Appropriateness criteria for active surveillance of prostate cancer. J Urol. 2017;197(1):67-74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
