

Health care use and costs at the end of life: a comparison of elderly Australian decedents with and without a cancer history
- PMID: 28637450
- PMCID: PMC5480123
- DOI: 10.1186/s12904-017-0213-0
Health care use and costs at the end of life: a comparison of elderly Australian decedents with and without a cancer history
Erratum in
-
Erratum to: BMC Palliative Care, Vol. 17.BMC Palliat Care. 2017 Oct 10;16(1):51. doi: 10.1186/s12904-017-0233-9. BMC Palliat Care. 2017. PMID: 29017489 Free PMC article. No abstract available.
Abstract
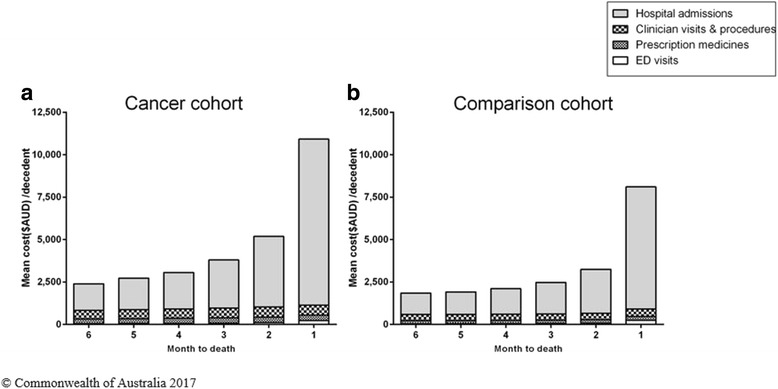
Background: There is limited population-level research on end-of-life care in Australia that considers health care use and costs across hospital and community sectors. The aim of this study was to quantify health care use and costs in the last 6 months of life in a cohort of elderly Australian decedents and to examine the factors associated with end-of-life resource use and costs.
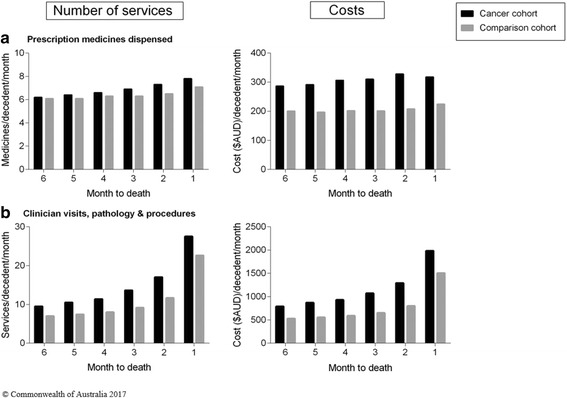
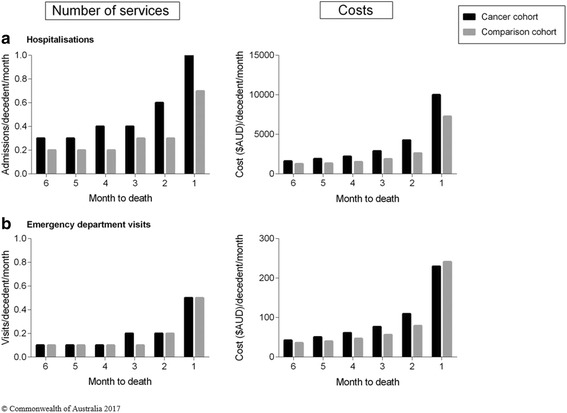
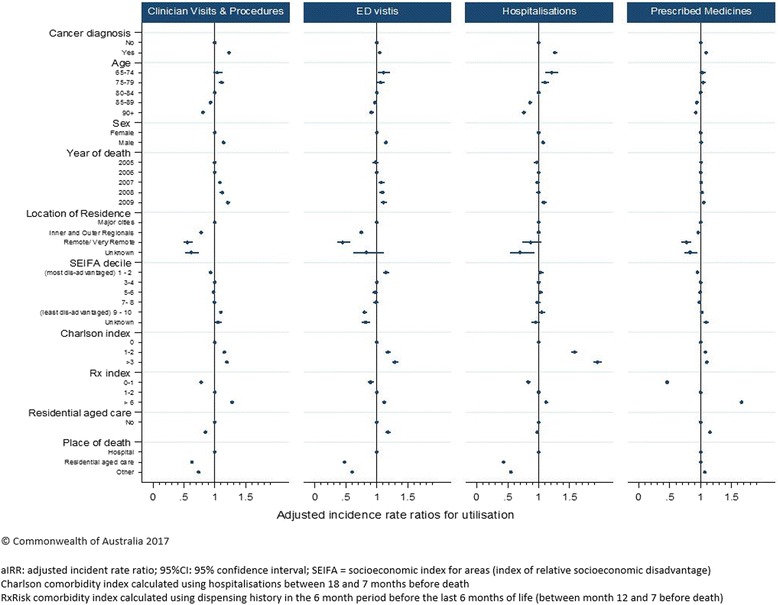
Methods: A retrospective cohort study using routinely collected health data from Australian Government Department of Veterans' Affairs clients. The study included two cohorts of elderly Australians who died between 2005 and 2009; one cohort with a recorded cancer diagnosis and a comparison cohort with no evidence of a cancer history. We examined hospitalisations, emergency department (ED) visits, prescription drugs, clinician visits, pathology, and procedures and associated costs in the last 6 months of life. We used negative binominal regression to explore factors associated with health service use and costs.
Results: The cancer cohort had significantly higher rates of health service use and 27% higher total health care costs than the comparison cohort; in both cohorts, costs were driven primarily by hospitalisations. Older age was associated with lower costs and those who died in residential aged care incurred half the costs of those who died in hospital.
Conclusions: The results suggest differences in end-of-life care pathways dependent on patient factors, with younger, community-dwelling patients and those with a history of cancer incurring significantly greater costs. There is a need to examine whether the investment in end-of-life care meets patient and societal needs.
Keywords: End-of-life care; Health care costs; Health care utilisation; Neoplasm; Terminal care; Veterans health.
Figures

References
-
- OECD . Economic, environmental and social statistics. Paris: OECD; 2009.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
