

Do COPD subtypes really exist? COPD heterogeneity and clustering in 10 independent cohorts
- PMID: 28637835
- PMCID: PMC6013053
- DOI: 10.1136/thoraxjnl-2016-209846
Do COPD subtypes really exist? COPD heterogeneity and clustering in 10 independent cohorts
Abstract
Background: COPD is a heterogeneous disease, but there is little consensus on specific definitions for COPD subtypes. Unsupervised clustering offers the promise of 'unbiased' data-driven assessment of COPD heterogeneity. Multiple groups have identified COPD subtypes using cluster analysis, but there has been no systematic assessment of the reproducibility of these subtypes.
Objective: We performed clustering analyses across 10 cohorts in North America and Europe in order to assess the reproducibility of (1) correlation patterns of key COPD-related clinical characteristics and (2) clustering results.
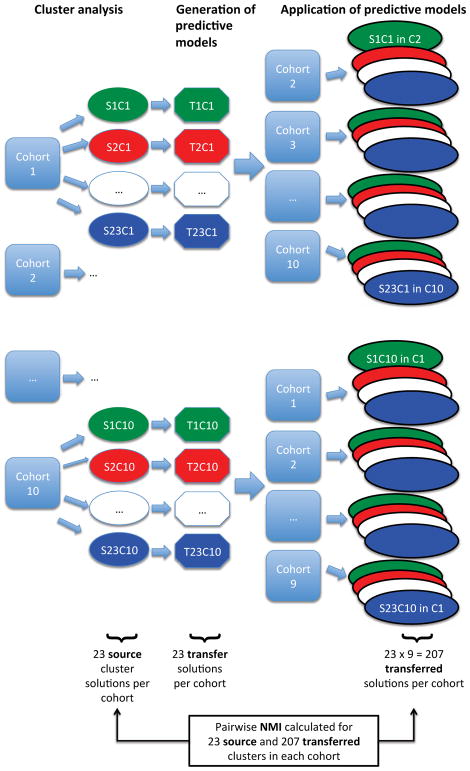
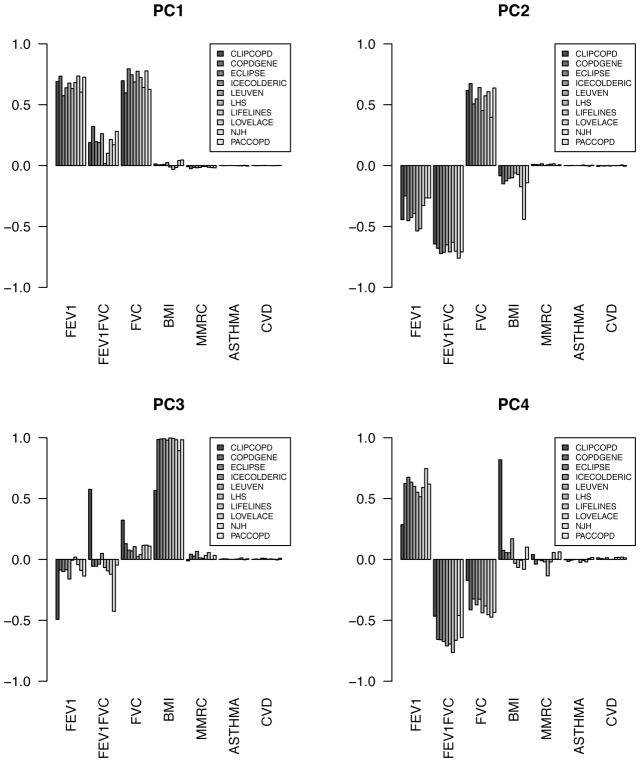
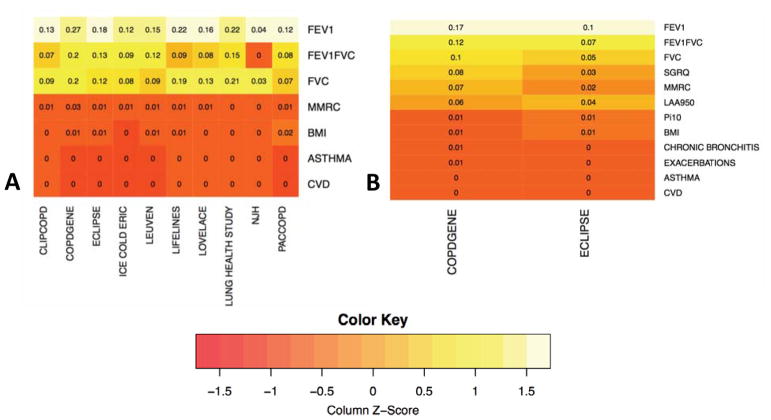
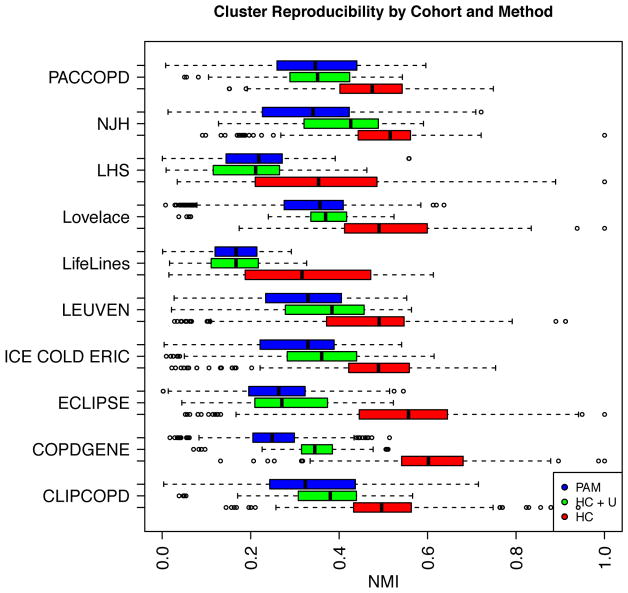
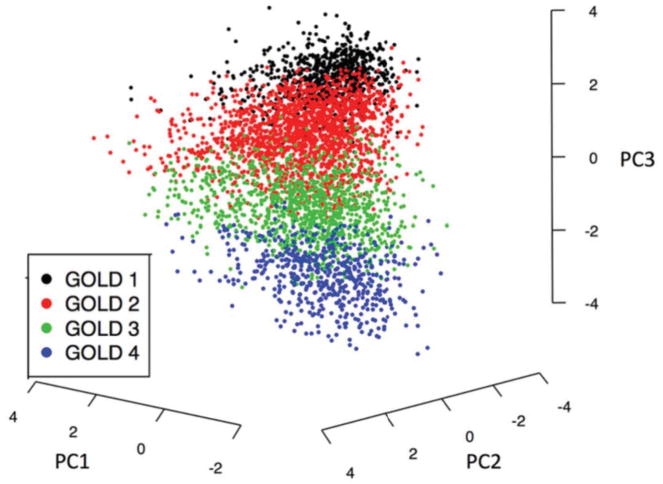
Methods: We studied 17 146 individuals with COPD using identical methods and common COPD-related characteristics across cohorts (FEV1, FEV1/FVC, FVC, body mass index, Modified Medical Research Council score, asthma and cardiovascular comorbid disease). Correlation patterns between these clinical characteristics were assessed by principal components analysis (PCA). Cluster analysis was performed using k-medoids and hierarchical clustering, and concordance of clustering solutions was quantified with normalised mutual information (NMI), a metric that ranges from 0 to 1 with higher values indicating greater concordance.
Results: The reproducibility of COPD clustering subtypes across studies was modest (median NMI range 0.17-0.43). For methods that excluded individuals that did not clearly belong to any cluster, agreement was better but still suboptimal (median NMI range 0.32-0.60). Continuous representations of COPD clinical characteristics derived from PCA were much more consistent across studies.
Conclusions: Identical clustering analyses across multiple COPD cohorts showed modest reproducibility. COPD heterogeneity is better characterised by continuous disease traits coexisting in varying degrees within the same individual, rather than by mutually exclusive COPD subtypes.
Keywords: COPD epidemiology.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: Over the past 3 years, PJC has received research support and consulting fees from GSK. Other authors have no competing interests to declare.
Figures
References
-
- Burgel P-R, Paillasseur J-L, Caillaud D, et al. Clinical COPD phenotypes: a novel approach using principal component and cluster analyses. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2010;36:531–9. doi: 10.1183/09031936.00175109. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical