

Multidisciplinary approach of colorectal cancer liver metastases
- PMID: 28638789
- PMCID: PMC5465009
- DOI: 10.5306/wjco.v8.i3.190
Multidisciplinary approach of colorectal cancer liver metastases
Abstract
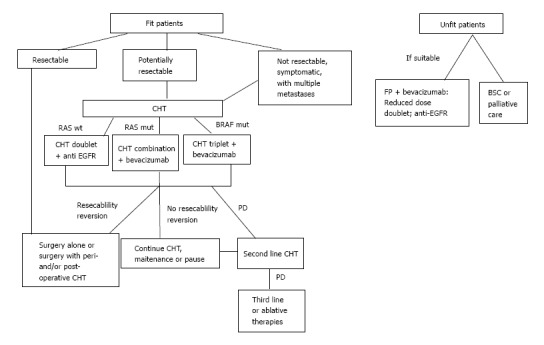
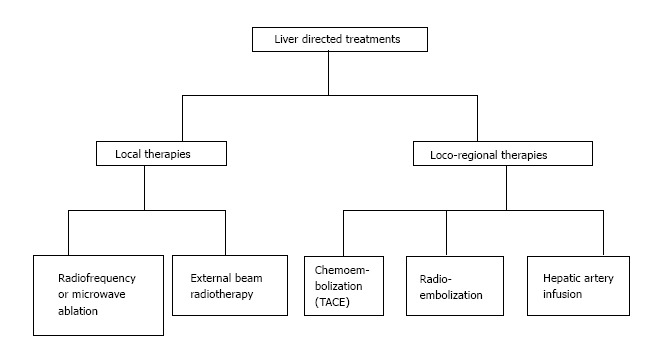
Large bowel cancer is a worldwide public health challenge. More than one third of patients present an advanced stage of disease at diagnosis and the liver is the most common site of metastases. Selection criteria for early diagnosis, chemotherapy and surgery have been recently expanded. The definition of resectability remains unclear. The presence of metastases is the most significant prognostic factor. For this reason the surgical resection of hepatic metastases is the leading treatment. The most appropriate resection approach remains to be defined. The two step and simultaneous resection processes of both primary and metastases have comparable survival long-term outcomes. The advent of targeted biological chemotherapeutic agents and the development of loco-regional therapies (chemoembolization, thermal ablation, arterial infusion chemotherapy) contribute to extend favorable results. Standardized evidence-based protocols are missing, hence optimal management of hepatic metastases should be single patient tailored and decided by a multidisciplinary team. This article reviews the outcomes of resection, systemic and loco-regional therapies of liver metastases originating from large bowel cancer.
Keywords: Arterial infusion chemotherapy; Chemoembolization; Chemotherapy; Colorectal cancer; Colorectal cancer liver metastases; Hepatic resection; Liver metastases; Radioembolization.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures
References
-
- World Health Organization. International Agency for Research in Cancer. Globocan 2012 estimated cancer incidence, mortality and prevalence worldwide 2012. [accessed 2016 Aug 20] Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx.
-
- Pawlik TM, Schulick RD, Choti MA. Expanding criteria for resectability of colorectal liver metastases. Oncologist. 2008;13:51–64. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
