

Leukodystrophies: a proposed classification system based on pathological changes and pathogenetic mechanisms
- PMID: 28638987
- PMCID: PMC5563342
- DOI: 10.1007/s00401-017-1739-1
Leukodystrophies: a proposed classification system based on pathological changes and pathogenetic mechanisms
Abstract
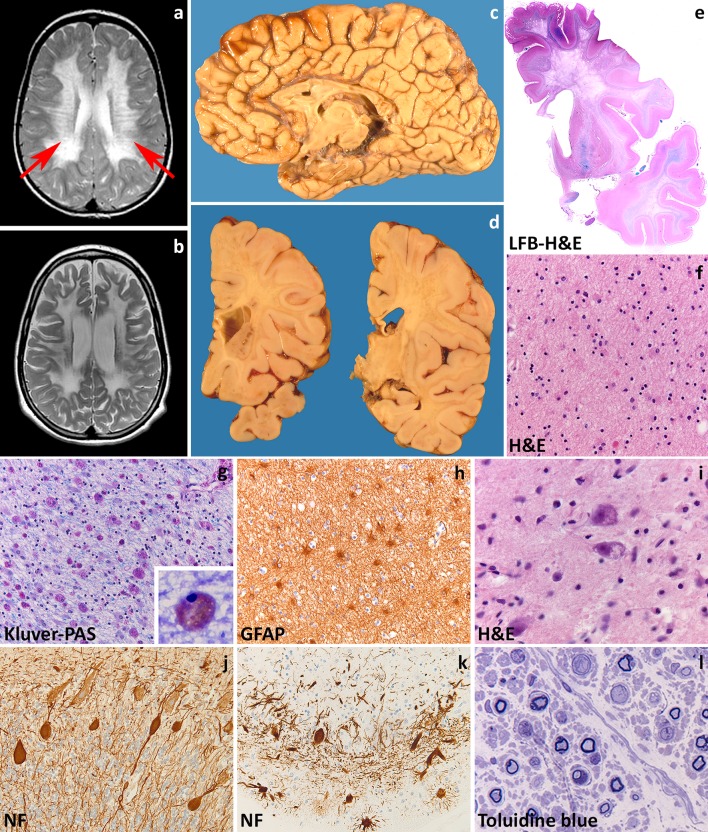
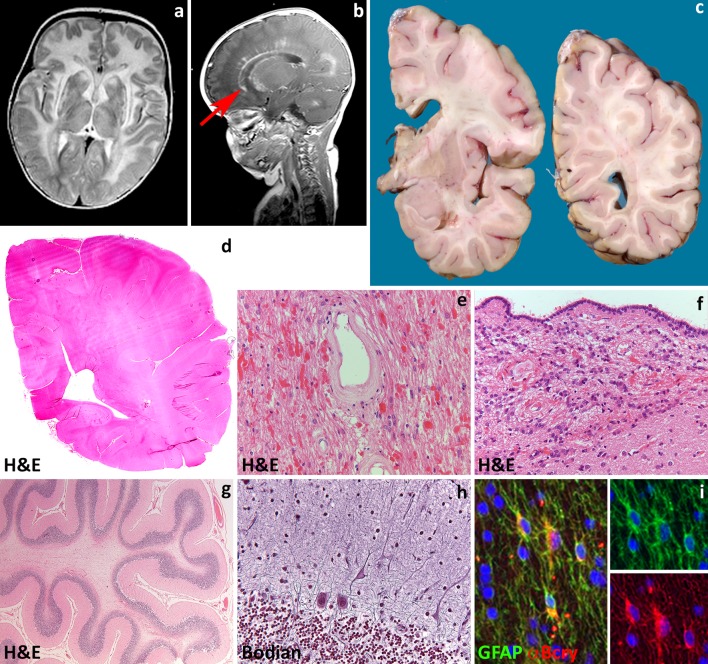
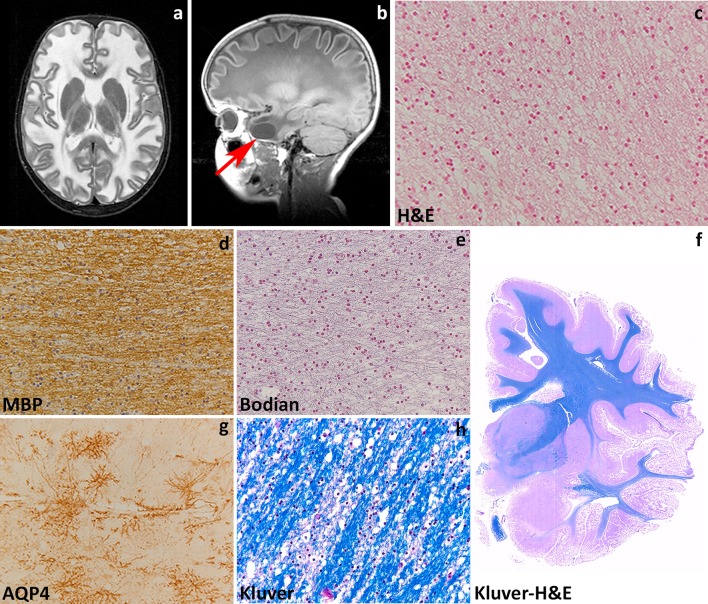
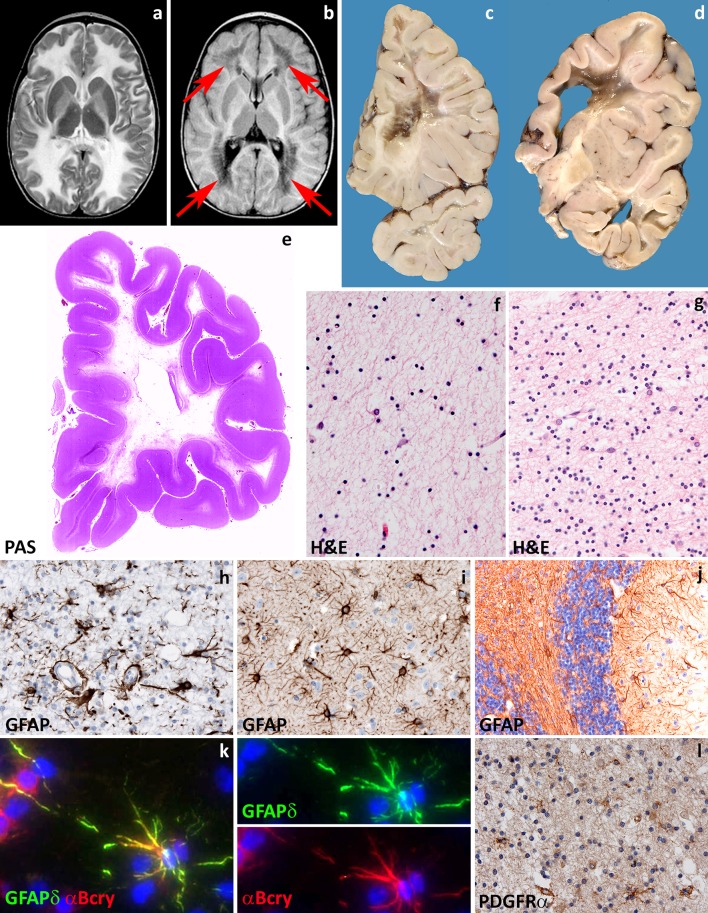
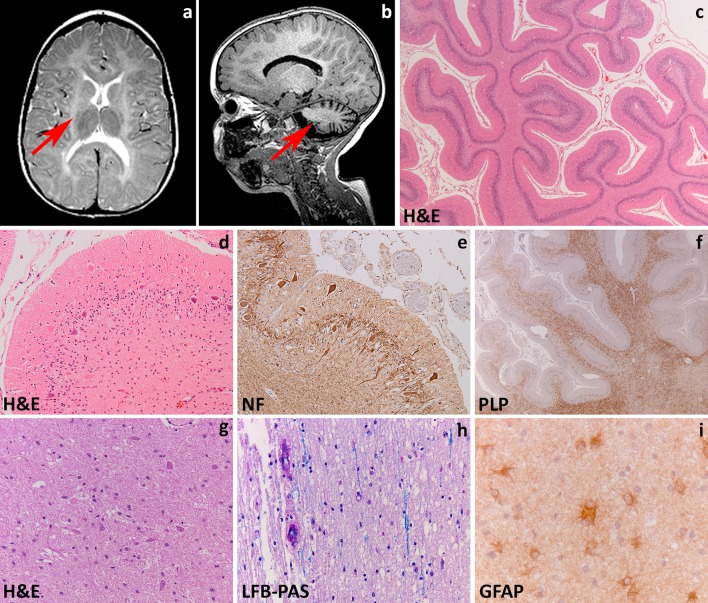
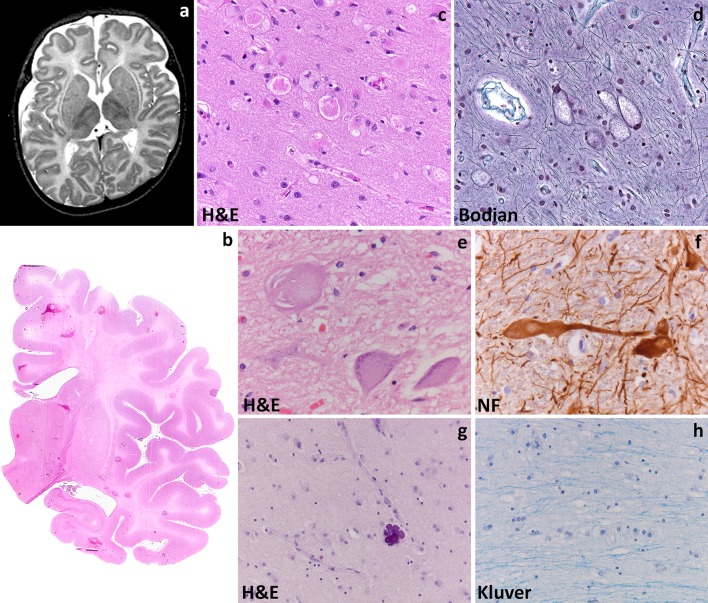
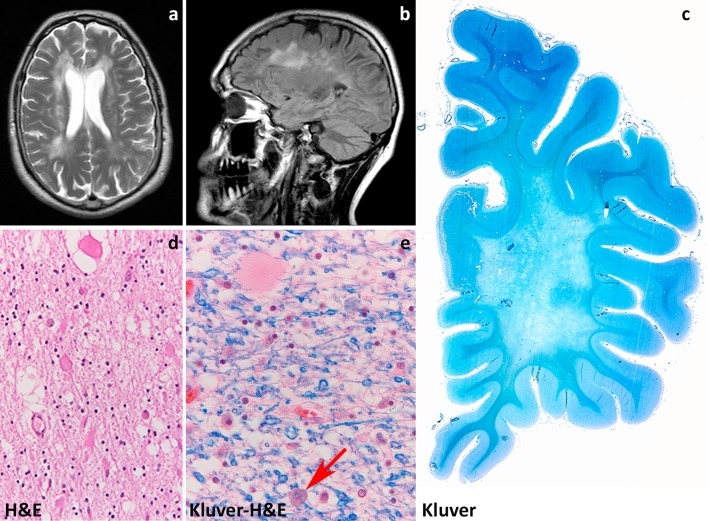
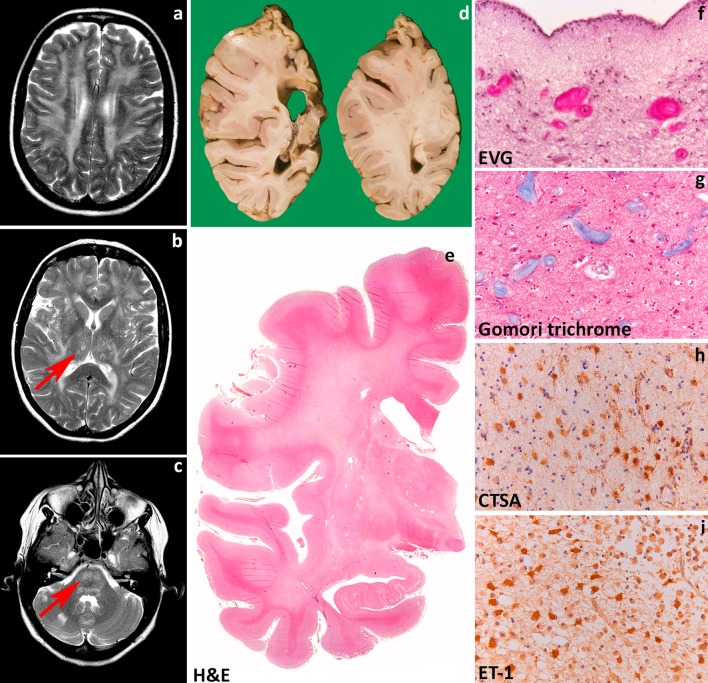
Leukodystrophies are genetically determined disorders characterized by the selective involvement of the central nervous system white matter. Onset may be at any age, from prenatal life to senescence. Many leukodystrophies are degenerative in nature, but some only impair white matter function. The clinical course is mostly progressive, but may also be static or even improving with time. Progressive leukodystrophies are often fatal, and no curative treatment is known. The last decade has witnessed a tremendous increase in the number of defined leukodystrophies also owing to a diagnostic approach combining magnetic resonance imaging pattern recognition and next generation sequencing. Knowledge on white matter physiology and pathology has also dramatically built up. This led to the recognition that only few leukodystrophies are due to mutations in myelin- or oligodendrocyte-specific genes, and many are rather caused by defects in other white matter structural components, including astrocytes, microglia, axons and blood vessels. We here propose a novel classification of leukodystrophies that takes into account the primary involvement of any white matter component. Categories in this classification are the myelin disorders due to a primary defect in oligodendrocytes or myelin (hypomyelinating and demyelinating leukodystrophies, leukodystrophies with myelin vacuolization); astrocytopathies; leuko-axonopathies; microgliopathies; and leuko-vasculopathies. Following this classification, we illustrate the neuropathology and disease mechanisms of some leukodystrophies taken as example for each category. Some leukodystrophies fall into more than one category. Given the complex molecular and cellular interplay underlying white matter pathology, recognition of the cellular pathology behind a disease becomes crucial in addressing possible treatment strategies.
Keywords: Astrocytes; Axons; Leukodystrophy; Microglia; Myelin; Oligodendrocytes.
Figures
References
-
- Agamanolis DP. Pathology & genetics. Developmental neuropathology. City: ISN Neuropath; 2004.
-
- Axelsson R, Roytta M, Sourander P, Akesson HO, Andersen O. Hereditary diffuse leucoencephalopathy with spheroids. Acta Psychiatr Scand Suppl. 1984;314:1–65. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
