

The G8 screening tool enhances prognostic value to ECOG performance status in elderly cancer patients: A retrospective, single institutional study
- PMID: 28640844
- PMCID: PMC5480957
- DOI: 10.1371/journal.pone.0179694
The G8 screening tool enhances prognostic value to ECOG performance status in elderly cancer patients: A retrospective, single institutional study
Abstract
Background: Some elderly cancer patients, even with good Eastern Cooperative Oncology Group performance status (ECOG-PS), have poor survival outcomes and cannot tolerate standard therapy. Few studies have detailed the associations between the G8 screening tool, ECOG-PS, and overall survival (OS) in such patients.
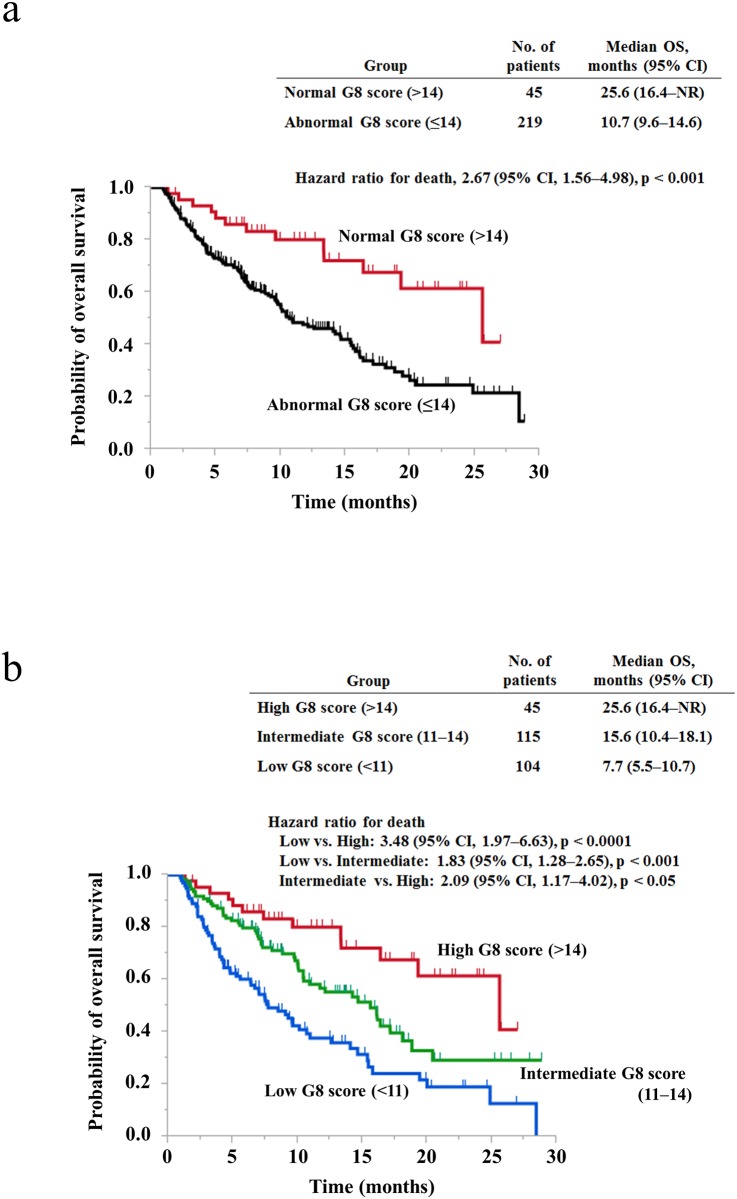
Methods: Cancer patients, aged 70 years or older, were assessed for G8 and classified into three groups according to their G8 score: <11 as the low score group, 11-14 as the intermediate score group, and >14 as the high score group. We retrospectively analyzed the association between G8 score and OS in all patients and for each ECOG-PS-categorized group.
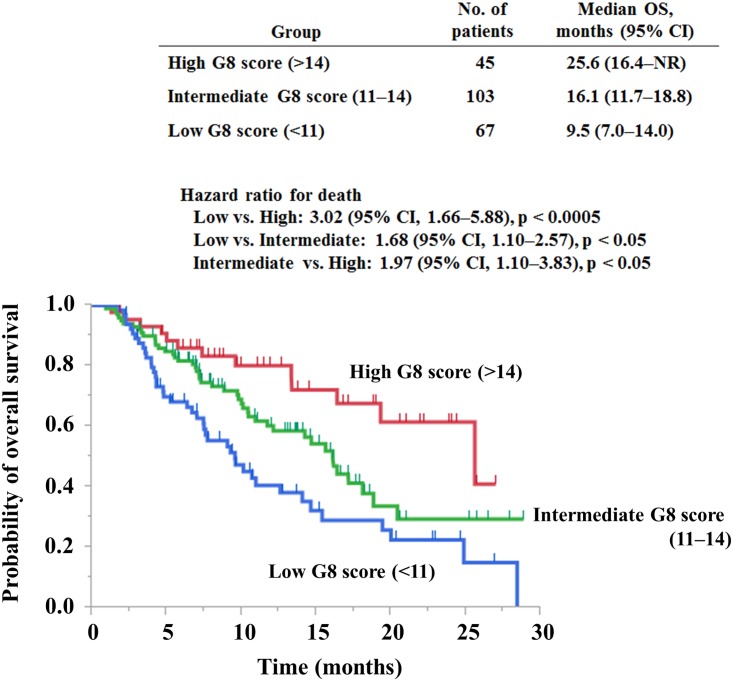
Results: Out of 264 enrolled patients, most patients (87%) with solid tumor were categorized as TNM stage IV. ECOG-PS was 0 or 1 in 215 patients and ≥2 in 48; there was missing data for one patient. Among all patients, the low score group with a median OS of 7.7 months survived significantly less than both the high score group with a median OS of 25.6 months [Hazard ratio (HR) 3.48; 95% confidence interval (CI), 1.96-6.63; p < 0.0001] and the intermediate score group with a median of 15.6 months (HR 1.83; 95% CI, 1.28-2.65; p < 0.001). In the multivariate analysis, TNM stage and G8 score were independent prognostic factors for OS. When patients with an ECOG-PS of 0 or 1 were analyzed, patients with a lower G8 score showed significantly shorter OS than patients with a higher score when any two groups were compared.
Conclusion: This novel classification of the G8 score contributes to prompt identification of patients with poor prognosis and improved the prognostic value of ECOG-PS. Using G8 with ECOG-PS may be helpful in deciding treatment for elderly patients with advanced cancer.
Conflict of interest statement
Figures
References
-
- Hori M, Matsuda T, Shibata A, Katanoda K, Sobue T, Nishimoto H. Cancer incidence and incidence rates in Japan in 2009: a study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol. 2015;45(9):884–91. doi: 10.1093/jjco/hyv088 . - DOI - PubMed
-
- Wildiers H, Heeren P, Puts M, Topinkova E, Janssen-Heijnen ML, Extermann M, et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J Clin Oncol. 2014;32(24):2595–603. doi: 10.1200/JCO.2013.54.8347 . - DOI - PMC - PubMed
-
- Puts MT, Hardt J, Monette J, Girre V, Springall E, Alibhai SM. Use of geriatric assessment for older adults in the oncology setting: a systematic review. J Natl Cancer Inst. 2012;104(15):1133–63. doi: 10.1093/jnci/djs285 . - DOI - PMC - PubMed
-
- Sattar S, Alibhai SM, Wildiers H, Puts MT. How to implement a geriatric assessment in your clinical practice. Oncologist. 2014;19(10):1056–68. doi: 10.1634/theoncologist.2014-0180 . - DOI - PMC - PubMed
-
- Bellera CA, Rainfray M, Mathoulin-Pelissier S, Mertens C, Delva F, Fonck M, et al. Screening older cancer patients: first evaluation of the G-8 geriatric screening tool. Ann Oncol. 2012;23(8):2166–72. doi: 10.1093/annonc/mdr587 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
