

Is self-assessment of medical abortion using a low-sensitivity pregnancy test combined with a checklist and phone text messages feasible in South African primary healthcare settings? A randomized trial
- PMID: 28640845
- PMCID: PMC5480887
- DOI: 10.1371/journal.pone.0179600
Is self-assessment of medical abortion using a low-sensitivity pregnancy test combined with a checklist and phone text messages feasible in South African primary healthcare settings? A randomized trial
Abstract
Objective: To evaluate feasibility of self-assessment of medical abortion outcome using a low-sensitivity urine pregnancy test, checklist and text messages. The study assessed whether accurate self-assessment required a demonstration of the low-sensitivity urine pregnancy test or if verbal instructions suffice.
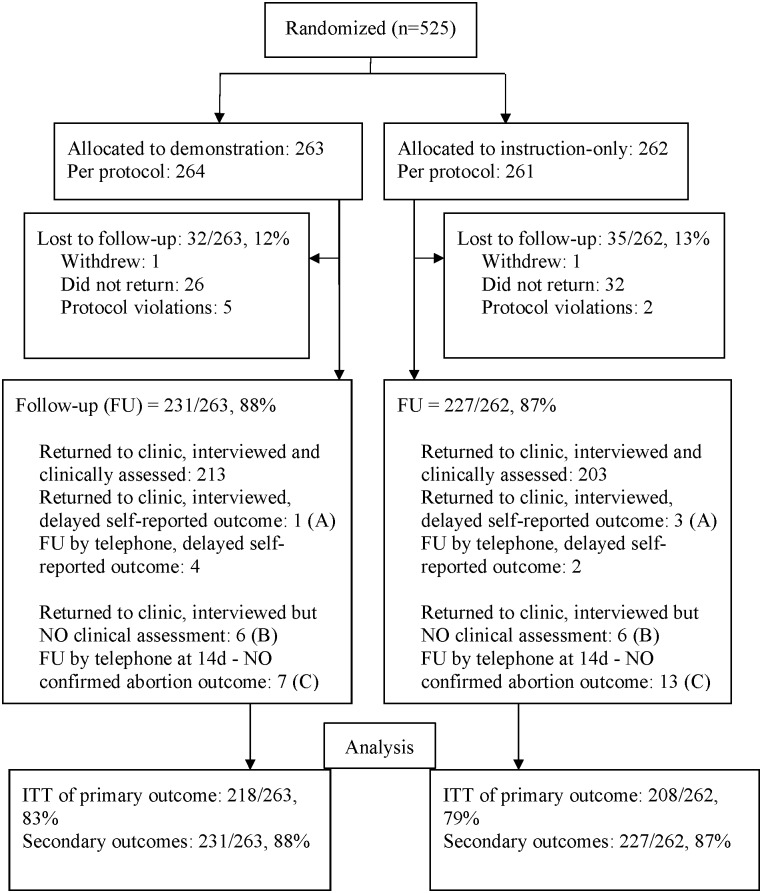
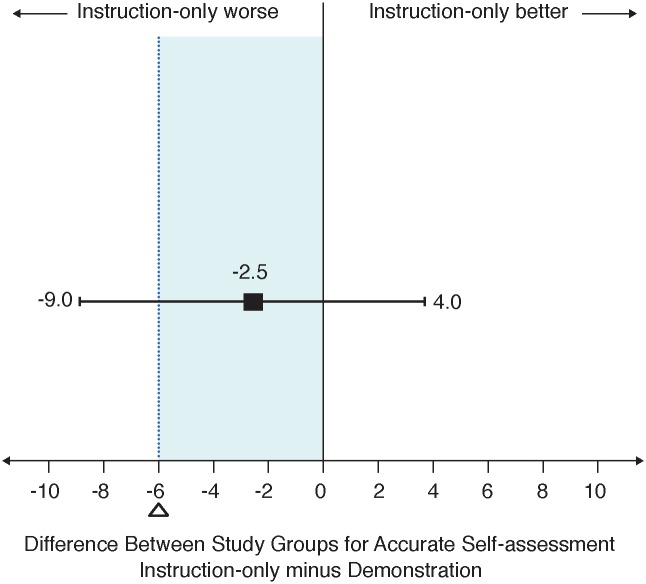
Methods: This non-inferiority trial enrolled 525 adult women from six public sector abortion clinics. Eligible women were undergoing medical abortion at gestations within 63 days. Consenting women completed a baseline interview, received standard care with mifepristone and home-administration of misoprostol. All were given a low-sensitivity urine pregnancy test and checklist for use 14 days later, sent text reminders, and asked to attend in-clinic follow-up after two weeks. Women were randomly assigned 1:1 to an instruction-only group (n = 262; issued with pre-scripted instructions on the low-sensitivity pregnancy test), or a demonstration group (n = 263; performed practice tests guided by lay health workers). The primary outcome was accurate self-assessment of incomplete abortion, defined as needing additional misoprostol or vacuum aspiration. Analysis was by intention to treat and a non-inferiority margin was set to six percentage points. Women's acceptability of their abortion procedure and preferences for follow-up were also assessed.
Results: Follow-up was 81% for abortion outcome, confirmed in-clinic at two weeks or self-reported within six months. Non-inferiority of instruction-only to a demonstration was inconclusive for accurate self-assessment (risk difference for instruction-only -demonstration: -2.5%; 95%CI: -9% to 4%). Comparing instruction-only to demonstration groups, 99% and 100% found the pregnancy test easy to do; and 91% and 93% respectively chose the pregnancy test, checklist and text messages for abortion outcome assessment in the future.
Conclusion: Routine self-assessment using a low-sensitivity pregnancy test, checklist and text messages is feasible and preferred by women attending South African primary care abortion clinics. Counselling with additional emphasis on prompt recognition of ongoing pregnancies is recommended.
Trial registration: ClinicalTrials.gov NCT02231619.
Conflict of interest statement
Figures
Similar articles
-
Mobile phone messages to provide support to women during the home phase of medical abortion in South Africa: a randomised controlled trial.Contraception. 2014 Sep;90(3):226-33. doi: 10.1016/j.contraception.2014.04.009. Epub 2014 Apr 24. Contraception. 2014. PMID: 24850188 Clinical Trial.
-
Self-assessment of the outcome of early medical abortion versus clinic follow-up in India: a randomised, controlled, non-inferiority trial.Lancet Glob Health. 2015 Sep;3(9):e537-45. doi: 10.1016/S2214-109X(15)00150-3. Lancet Glob Health. 2015. PMID: 26275330 Clinical Trial.
-
Acceptability and feasibility of phone follow-up with a semiquantitative urine pregnancy test after medical abortion in Moldova and Uzbekistan.Contraception. 2015 Feb;91(2):178-83. doi: 10.1016/j.contraception.2014.11.004. Epub 2014 Nov 15. Contraception. 2015. PMID: 25497383 Clinical Trial.
-
Follow-up strategies to confirm the success of medical abortion of pregnancies up to 10 weeks' gestation: a systematic review with meta-analyses.Am J Obstet Gynecol. 2020 Jun;222(6):551-563.e13. doi: 10.1016/j.ajog.2019.11.1244. Epub 2019 Nov 9. Am J Obstet Gynecol. 2020. PMID: 31715147
-
Effectiveness, safety and acceptability of self-assessment of the outcome of first-trimester medical abortion: a systematic review and meta-analysis.BJOG. 2019 Dec;126(13):1536-1544. doi: 10.1111/1471-0528.15922. Epub 2019 Sep 18. BJOG. 2019. PMID: 31471989
Cited by
-
Preimplantation genetic testing to reduce preterm births in assisted reproductive technology.Int J Gynaecol Obstet. 2020 Jul;150(1):34-40. doi: 10.1002/ijgo.13192. Int J Gynaecol Obstet. 2020. PMID: 32524593 Review.
-
Self-testing for pregnancy: a systematic review and meta-analysis.BMJ Open. 2022 Feb 28;12(2):e054120. doi: 10.1136/bmjopen-2021-054120. BMJ Open. 2022. PMID: 35228285 Free PMC article.
-
Exploring acceptability, opportunities, and challenges of community-based home pregnancy testing for early antenatal care initiation in rural Kenya.BMC Public Health. 2024 Jun 29;24(1):1742. doi: 10.1186/s12889-024-19254-7. BMC Public Health. 2024. PMID: 38951787 Free PMC article.
-
How task-sharing in abortion care became the norm in Sweden: A case study of historic and current determinants and events.Int J Gynaecol Obstet. 2020 Jul;150 Suppl 1(Suppl 1):34-42. doi: 10.1002/ijgo.13003. Int J Gynaecol Obstet. 2020. PMID: 33219992 Free PMC article.
-
The EQ-5D-3L administered by text message compared to the paper version for hard-to-reach populations in a rural South African trauma setting: a measurement equivalence study.Arch Orthop Trauma Surg. 2021 Jun;141(6):947-957. doi: 10.1007/s00402-020-03574-5. Epub 2020 Aug 12. Arch Orthop Trauma Surg. 2021. PMID: 32785761 Free PMC article.
References
-
- WCDOH. Provinical Policy Standardized Guidelines and Protocols on the Termination of Pregnancy Services. Cape Town, South Africa: Western Cape Department of Health; 2010.
-
- Raymond EG, Shannon C, Weaver MA, Winikoff B. First-trimester medical abortion with mifepristone 200 mg and misoprostol: a systematic review. Contraception. 2013;87(1):26–37. doi: 10.1016/j.contraception.2012.06.011 - DOI - PubMed
-
- Iyengar K, Paul M, Iyengar SD, Klingberg-Allvin M, Essén B, Bring J, et al. Self-assessment of the outcome of early medical abortion versus clinic follow-up in India: a randomised, controlled, non-inferiority trial. Lancet Global Health. 2015;3(9):e537–e45. doi: 10.1016/S2214-109X(15)00150-3 - DOI - PubMed
-
- Cameron ST, Glasier A, Johnstone A, Dewart H, Campbell A. Can women determine the success of early medical termination of pregnancy themselves? Contraception. 2015;91(1):6–11. doi: 10.1016/j.contraception.2014.09.009 - DOI - PubMed
-
- Oppegaard KS, Qvigstad E, Fiala C, Heikinheimo O, Benson L, Gemzell-Danielsson K. Clinical follow-up compared with self-assessment of outcome after medical abortion: a multicentre, non-inferiority, randomised, controlled trial. Lancet. 2014;385(9969):698–704. doi: 10.1016/S0140-6736(14)61054-0 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
