

Systematic review and meta-analysis of initial management of pneumothorax in adults: Intercostal tube drainage versus other invasive methods
- PMID: 28640890
- PMCID: PMC5480863
- DOI: 10.1371/journal.pone.0178802
Systematic review and meta-analysis of initial management of pneumothorax in adults: Intercostal tube drainage versus other invasive methods
Abstract
Objectives: The ideal invasive management as initial approach for pneumothorax (PTX) is still under debate. The purpose of this systematic review and meta-analysis was to examine the evidence for the effectiveness of intercostal tube drainage and other various invasive methods as the initial approach to all subtypes of PTX in adults.
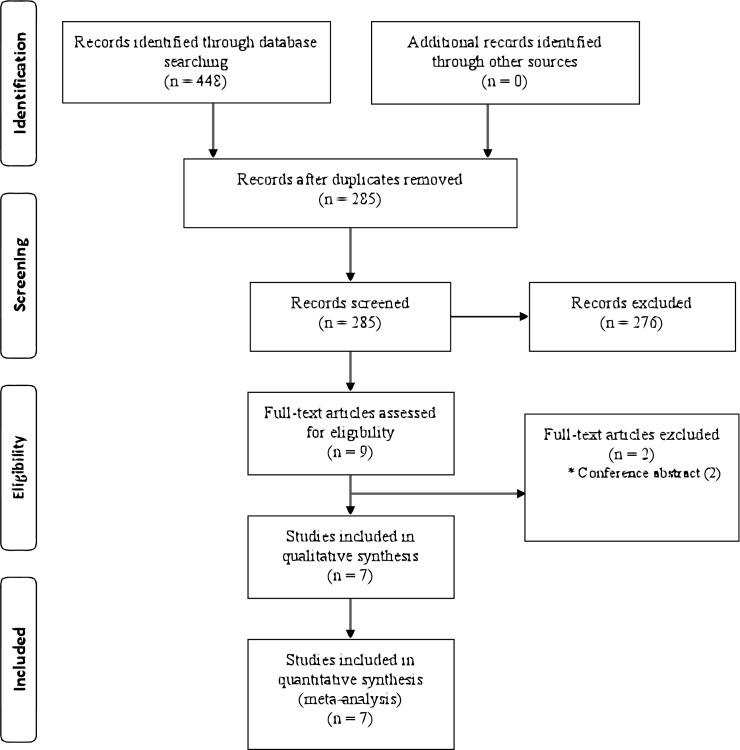
Methods: Three databases were searched from inception to May 29, 2016: MEDLINE, EMBASE, and the Cochrane CENTRAL. Randomised controlled trials that evaluated intercostal tube drainage as the control and various invasive methods as the intervention for the initial approach to PTX in adults were included. The primary outcome was the early success rate of each method, and the risk ratios (RRs) were used for an effect size measure. The secondary outcomes were recurrence rate, hospitalization rate, hospital stay, and complications.
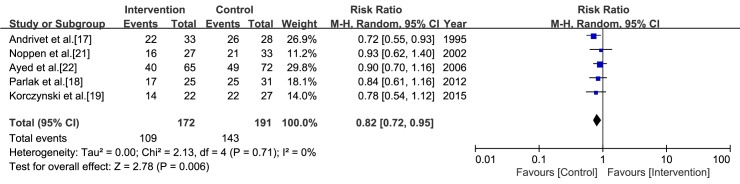
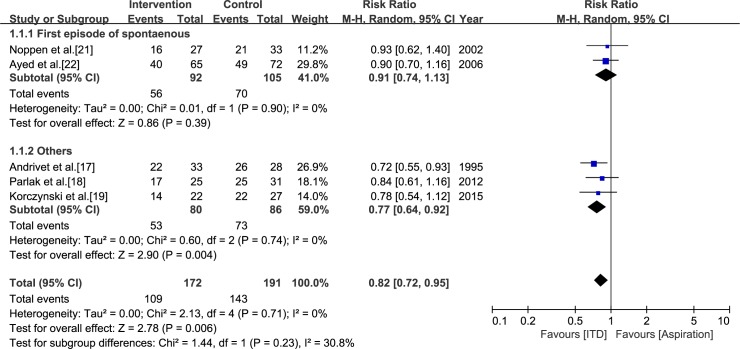
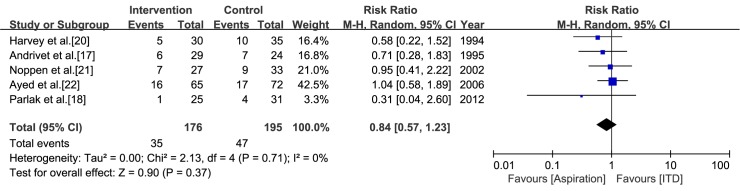
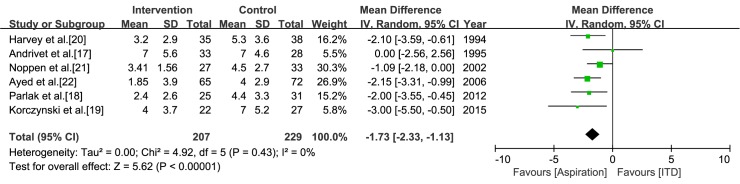
Results: Seven studies met our inclusion criteria. Interventions were aspiration in six studies and catheterization connected to a one-way valve in one study. Meta-analyses were conducted for early success rate, recurrence rate, hospitalization rate, and hospital stay. Aspiration was inferior to intercostal tube drainage in terms of early success rate (RR = 0.82, confidence interval [CI] = 0.72 to 0.95, I2 = 0%). While aspiration and intercostal tube drainage showed no significant difference in the recurrence rate (RR = 0.84, CI = 0.57 to 1.23, I2 = 0%), aspiration had shorter hospital stay than intercostal tube drainage (mean difference = -1.73, CI = -2.33 to -1.13, I2 = 0%). Aspiration had lower hospitalization rate than intercostal tube drainage, but marked heterogeneity was present (RR = 0.38, CI = 0.19 to 0.76, I2 = 85%).
Conclusion: Aspiration was inferior to intercostal tube drainage in terms of early resolution, but it had shorter hospital stay. The recurrence rate of aspiration and intercostal tube drainage did not differ significantly. The efficacy of catheterization connected to a one-way valve was inconclusive because of the small number of relevant studies. (Registration of study protocol: PROSPERO, CRD42016037866).
Conflict of interest statement
Figures

References
-
- Bense L, Eklund G, Wiman LG. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest. 1987;92: 1009–1012 - PubMed
-
- Melton LJ, 3rd, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. Am Rev Respir Dis. 1979;120: 1379–1382. doi: 10.1164/arrd.1979.120.6.1379 - DOI - PubMed
-
- Gupta D, Hansell A, Nichols T, Duong T, Ayres JG, Strachan D. Epidemiology of pneumothorax in England. Thorax. 2000;55: 666–671 doi: 10.1136/thorax.55.8.666 - DOI - PMC - PubMed
-
- Schramel FM, Postmus PE, Vanderschueren RG. Current aspects of spontaneous pneumothorax. Eur Respir J. 1997;10: 1372–1379 - PubMed
-
- Chambers A, Scarci M. In patients with first-episode primary spontaneous pneumothorax is video-assisted thoracoscopic surgery superior to tube thoracostomy alone in terms of time to resolution of pneumothorax and incidence of recurrence? Interact Cardiovasc Thorac Surg. 2009;9: 1003–1008. doi: 10.1510/icvts.2009.216473 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
