

The value of visual field testing in the era of advanced imaging: clinical and psychophysical perspectives
- PMID: 28640951
- PMCID: PMC5519947
- DOI: 10.1111/cxo.12551
The value of visual field testing in the era of advanced imaging: clinical and psychophysical perspectives
Abstract
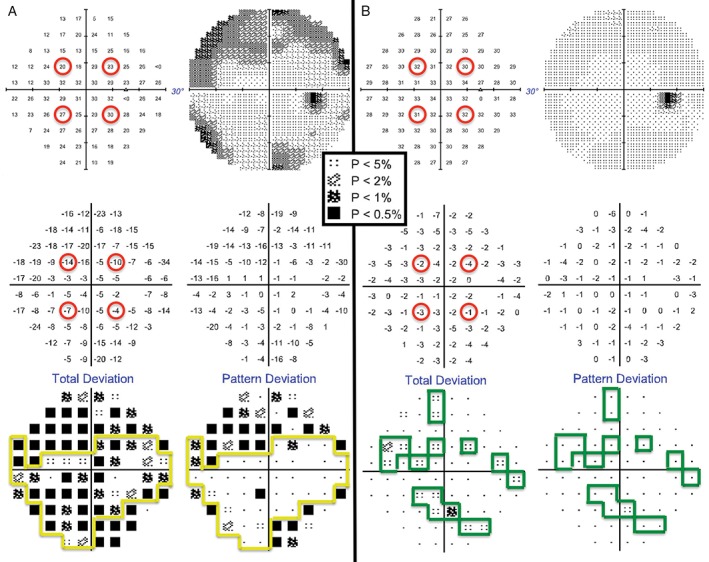
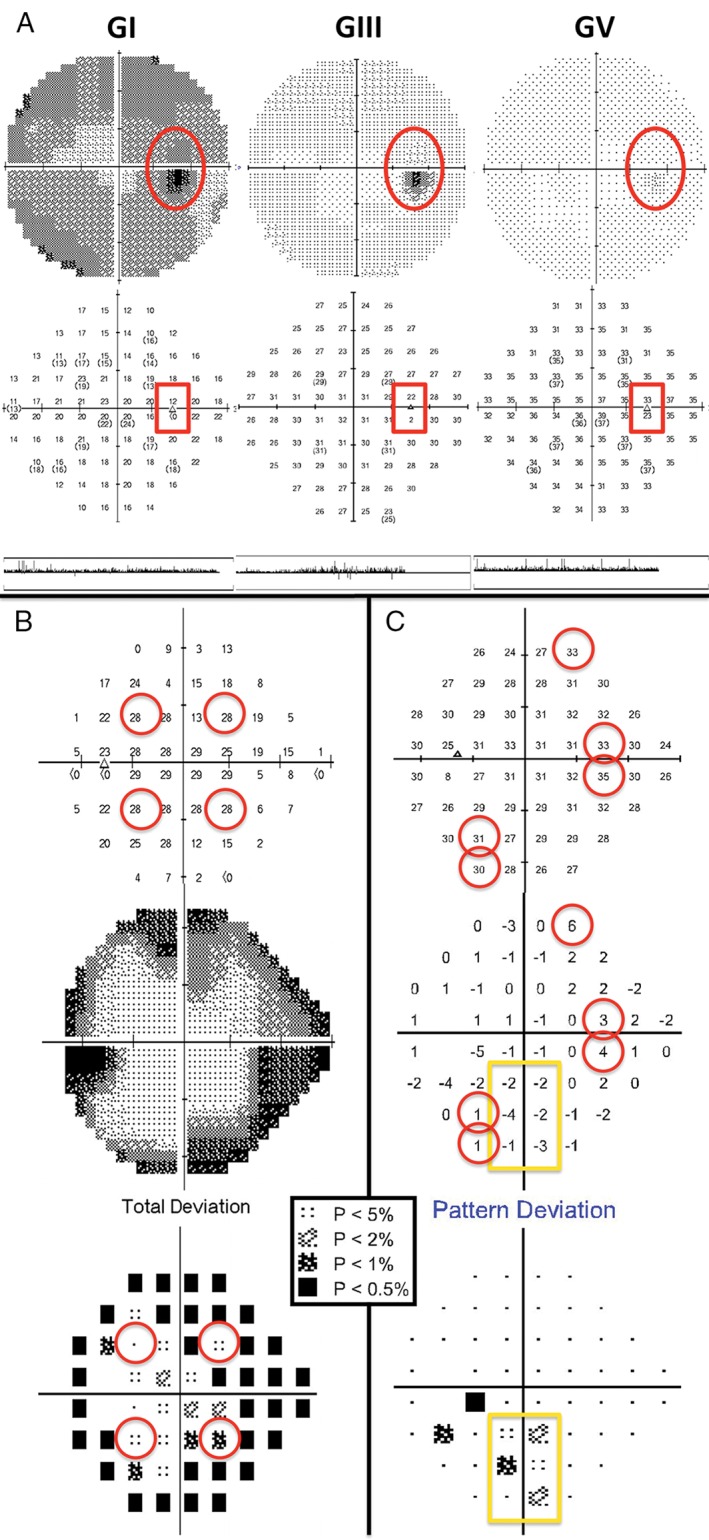
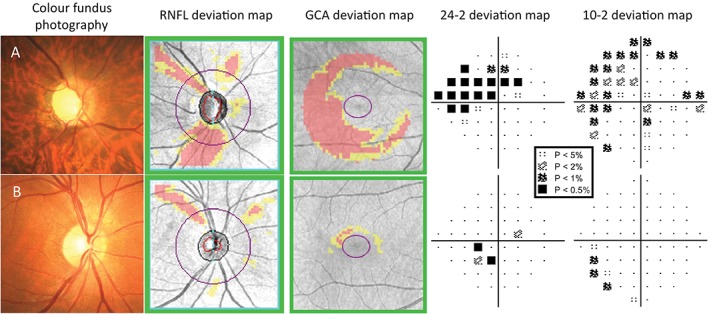
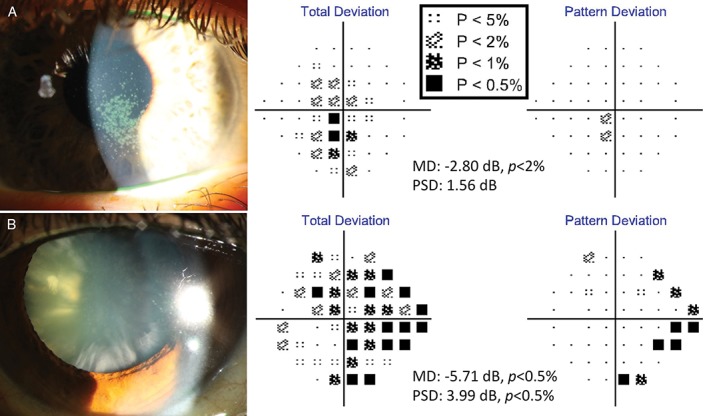
White-on-white standard automated perimetry (SAP) is widely used in clinical and research settings for assessment of contrast sensitivity using incremental light stimuli across the visual field. It is one of the main functional measures of the effect of disease upon the visual system. SAP has evolved over the last 40 years to become an indispensable tool for comprehensive assessment of visual function. In modern clinical practice, a range of objective measurements of ocular structure, such as optical coherence tomography, have also become invaluable additions to the arsenal of the ophthalmic examination. Although structure-function correlation is a highly desirable determinant of an unambiguous clinical picture for a patient, in practice, clinicians are often faced with discordance of structural and functional results, which presents them with a challenge. The construction principles behind the development of SAP are used to discuss the interpretation of visual fields, as well as the problem of structure-function discordance. Through illustrative clinical examples, we provide useful insights to assist clinicians in combining a range of clinical results obtained from SAP and from advanced imaging techniques into a coherent picture that can help direct clinical management.
Keywords: Bloch's law; Ricco's law; glaucoma; optical coherence tomography; perimetry; psychophysics; spatial summation; structure-function; temporal summation; tilted disc syndrome.
© 2017 The Authors. Clinical and Experimental Optometry published by John Wiley & Sons Australia, Ltd on behalf of Optometry Australia.
Figures
References
-
- Traquair HM. An Introduction to Clinical Perimetry. London: Henry Kimpton, 1927.
-
- Schiefer U, Patzold J, Dannheim F. [Conventional techniques of visual field examination Part 2: confrontation visual field testing ‐ kinetic perimetry]. Ophthalmologe 2005; 102: 821–827. - PubMed
-
- Spector RH. Visual fields In: Walker HK, Wall WD, Hurst JW. eds. Clinical Methods: The History, Physical and Laboratory Examinations, 3rd edn. Boston: Butterworths, 1990. - PubMed
-
- Khuu SK, Kalloniatis M. Standard automated perimetry: determining spatial summation and its effect on contrast sensitivity across the visual field. Invest Ophthalmol Vis Sci 2015; 56: 3565–3576. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous