

Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial
- PMID: 28642008
- PMCID: PMC5555437
- DOI: 10.1016/S1470-2045(17)30318-2
Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial
Abstract
Background: Concurrent chemoradiotherapy is the standard of care in limited-stage small-cell lung cancer, but the optimal radiotherapy schedule and dose remains controversial. The aim of this study was to establish a standard chemoradiotherapy treatment regimen in limited-stage small-cell lung cancer.
Methods: The CONVERT trial was an open-label, phase 3, randomised superiority trial. We enrolled adult patients (aged ≥18 years) who had cytologically or histologically confirmed limited-stage small-cell lung cancer, Eastern Cooperative Oncology Group performance status of 0-2, and adequate pulmonary function. Patients were recruited from 73 centres in eight countries. Patients were randomly assigned to receive either 45 Gy radiotherapy in 30 twice-daily fractions of 1·5 Gy over 19 days, or 66 Gy in 33 once-daily fractions of 2 Gy over 45 days, starting on day 22 after commencing cisplatin-etoposide chemotherapy (given as four to six cycles every 3 weeks in both groups). The allocation method used was minimisation with a random element, stratified by institution, planned number of chemotherapy cycles, and performance status. Treatment group assignments were not masked. The primary endpoint was overall survival, defined as time from randomisation until death from any cause, analysed by modified intention-to-treat. A 12% higher overall survival at 2 years in the once-daily group versus the twice-daily group was considered to be clinically significant to show superiority of the once-daily regimen. The study is registered with ClinicalTrials.gov (NCT00433563) and is currently in follow-up.
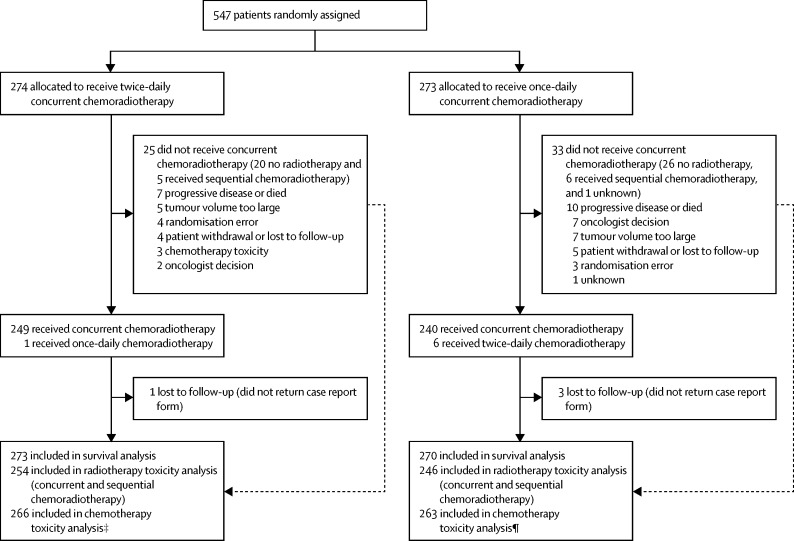
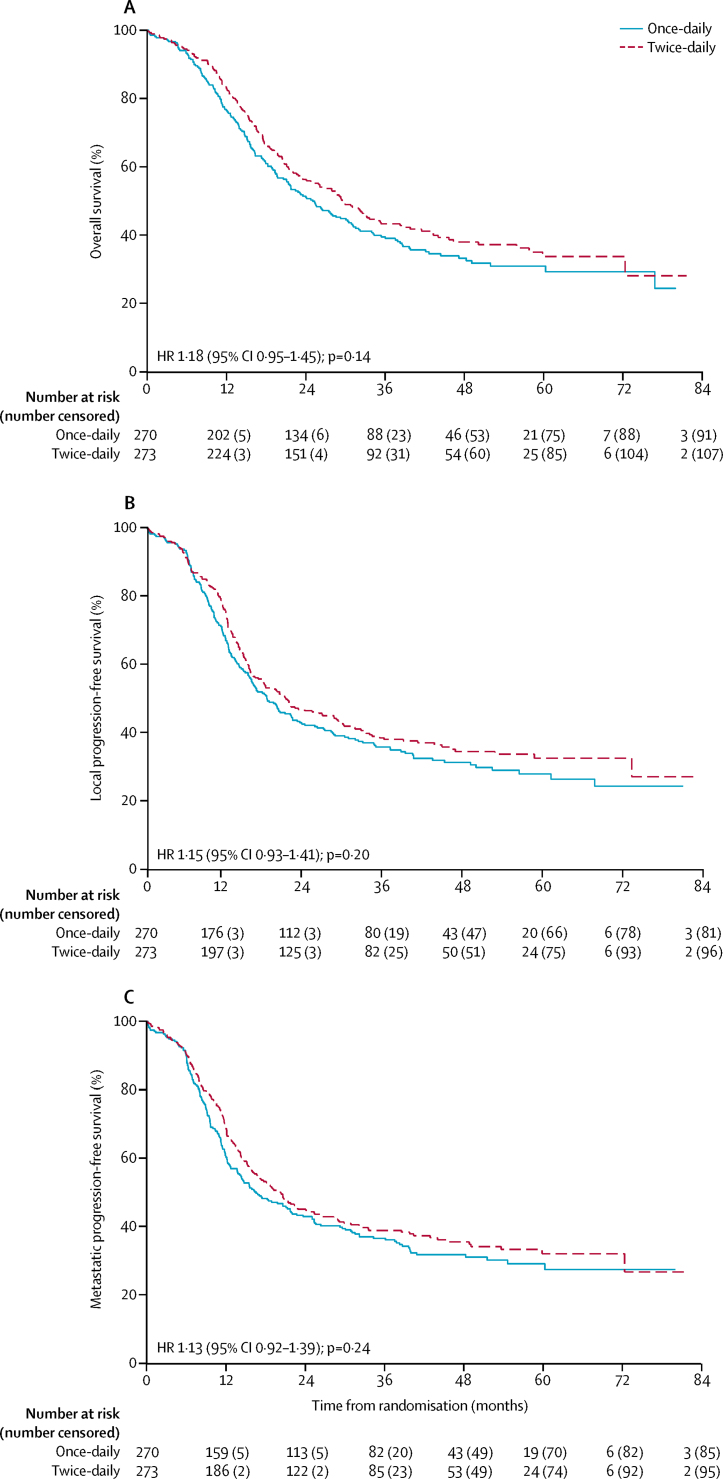
Findings: Between April 7, 2008, and Nov 29, 2013, 547 patients were enrolled and randomly assigned to receive twice-daily concurrent chemoradiotherapy (274 patients) or once-daily concurrent chemoradiotherapy (273 patients). Four patients (one in the twice-daily group and three in the once-daily group) did not return their case report forms and were lost to follow-up; these patients were not included in our analyses. At a median follow-up of 45 months (IQR 35-58), median overall survival was 30 months (95% CI 24-34) in the twice-daily group versus 25 months (21-31) in the once-daily group (hazard ratio for death in the once daily group 1·18 [95% CI 0·95-1·45]; p=0·14). 2-year overall survival was 56% (95% CI 50-62) in the twice-daily group and 51% (45-57) in the once-daily group (absolute difference between the treatment groups 5·3% [95% CI -3·2% to 13·7%]). The most common grade 3-4 adverse event in patients evaluated for chemotherapy toxicity was neutropenia (197 [74%] of 266 patients in the twice-daily group vs 170 [65%] of 263 in the once-daily group). Most toxicities were similar between the groups, except there was significantly more grade 4 neutropenia with twice-daily radiotherapy (129 [49%] vs 101 [38%]; p=0·05). In patients assessed for radiotherapy toxicity, was no difference in grade 3-4 oesophagitis between the groups (47 [19%] of 254 patients in the twice-daily group vs 47 [19%] of 246 in the once-daily group; p=0·85) and grade 3-4 radiation pneumonitis (4 [3%] of 254 vs 4 [2%] of 246; p=0·70). 11 patients died from treatment-related causes (three in the twice-daily group and eight in the once-daily group).
Interpretation: Survival outcomes did not differ between twice-daily and once-daily concurrent chemoradiotherapy in patients with limited-stage small-cell lung cancer, and toxicity was similar and lower than expected with both regimens. Since the trial was designed to show superiority of once-daily radiotherapy and was not powered to show equivalence, the implication is that twice-daily radiotherapy should continue to be considered the standard of care in this setting.
Funding: Cancer Research UK (Clinical Trials Awards and Advisory Committee), French Ministry of Health, Canadian Cancer Society Research Institute, European Organisation for Research and Treatment of Cancer (Cancer Research Fund, Lung Cancer, and Radiation Oncology Groups).
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC-BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Which fractionation of radiotherapy is best for limited-stage small-cell lung cancer?Lancet Oncol. 2017 Aug;18(8):994-995. doi: 10.1016/S1470-2045(17)30439-4. Epub 2017 Jun 20. Lancet Oncol. 2017. PMID: 28642007 No abstract available.
-
Is it time to convert the frequency of radiotherapy in small-cell lung cancer?Lancet Oncol. 2017 Oct;18(10):e553. doi: 10.1016/S1470-2045(17)30580-6. Lancet Oncol. 2017. PMID: 28971812 No abstract available.
-
Is it time to convert the frequency of radiotherapy in small-cell lung cancer?Lancet Oncol. 2017 Oct;18(10):e554. doi: 10.1016/S1470-2045(17)30581-8. Lancet Oncol. 2017. PMID: 28971813 No abstract available.
-
Is it time to convert the frequency of radiotherapy in small-cell lung cancer?Lancet Oncol. 2017 Oct;18(10):e555. doi: 10.1016/S1470-2045(17)30620-4. Lancet Oncol. 2017. PMID: 28971814 No abstract available.
-
Is it time to convert the frequency of radiotherapy in small-cell lung cancer? - Authors' reply.Lancet Oncol. 2017 Oct;18(10):e556. doi: 10.1016/S1470-2045(17)30611-3. Lancet Oncol. 2017. PMID: 28971815 No abstract available.
-
[Concurrent once-daily or twice-daily chemoradiotherapy in limited-stage small-cell lung cancer?].Strahlenther Onkol. 2018 Jan;194(1):73-75. doi: 10.1007/s00066-017-1234-6. Strahlenther Onkol. 2018. PMID: 29143097 German. No abstract available.
-
CONVERTed or not: what are the barriers to implementing the evidence?Lancet Oncol. 2017 Nov;18(11):e627. doi: 10.1016/S1470-2045(17)30808-2. Epub 2017 Oct 31. Lancet Oncol. 2017. PMID: 29208381 No abstract available.
-
CONVERTed or not: what are the barriers to implementing the evidence? - Author's reply.Lancet Oncol. 2017 Nov;18(11):e628. doi: 10.1016/S1470-2045(17)30800-8. Epub 2017 Oct 31. Lancet Oncol. 2017. PMID: 29208382 No abstract available.
-
Twice-daily chemoradiotherapy must still be the choice for patients with limited-stage small-cell lung cancer.J Thorac Dis. 2017 Sep;9(9):2843-2846. doi: 10.21037/jtd.2017.08.113. J Thorac Dis. 2017. PMID: 29221253 Free PMC article. No abstract available.
References
-
- Govindan R, Page N, Morgensztern D. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24:4539–4544. - PubMed
-
- Murray N, Coy P, Pater JL. Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 1993;11:336–344. - PubMed
-
- Johnson BE, Bridges JD, Sobczeck M. Patients with limited-stage small-cell lung cancer treated with concurrent twice-daily chest radiotherapy and etoposide/cisplatin followed by cyclophosphamide, doxorubicin, and vincristine. J Clin Oncol. 1996;14:806–813. - PubMed
-
- Turrisi AT, Kim K, Blum R. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med. 1999;340:265–271. - PubMed
-
- Pignon JP, Arriagada R, Ihde DC. A meta-analysis of thoracic radiotherapy for small-cell lung cancer. N Engl J Med. 1992;327:1618–1624. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
