

Coronary microvascular dysfunction in diabetes mellitus
- PMID: 28643578
- PMCID: PMC5805190
- DOI: 10.1177/0300060516675504
Coronary microvascular dysfunction in diabetes mellitus
Abstract
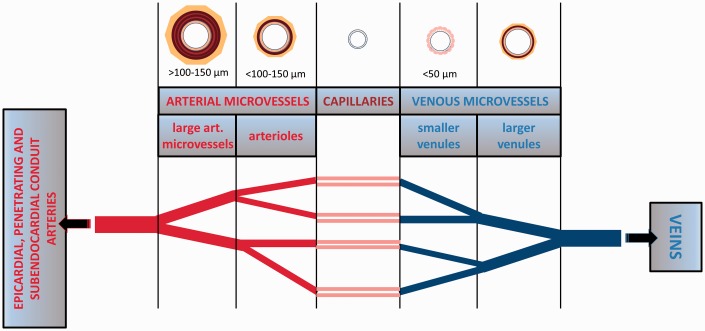
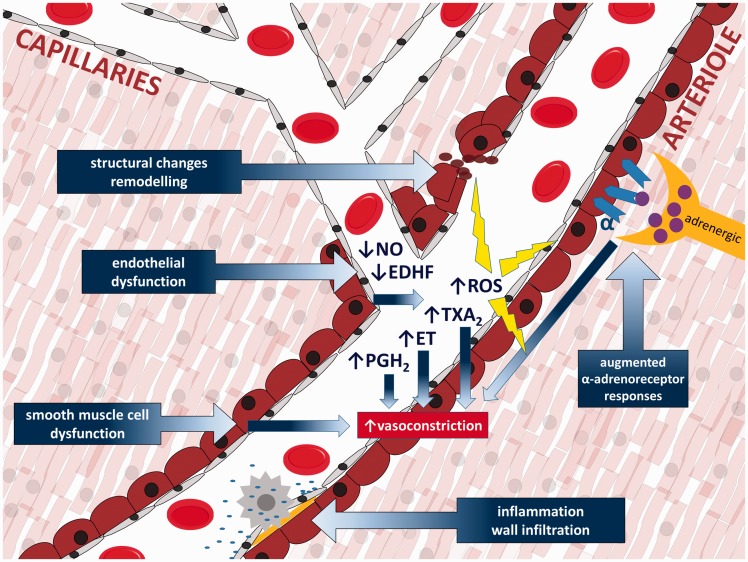
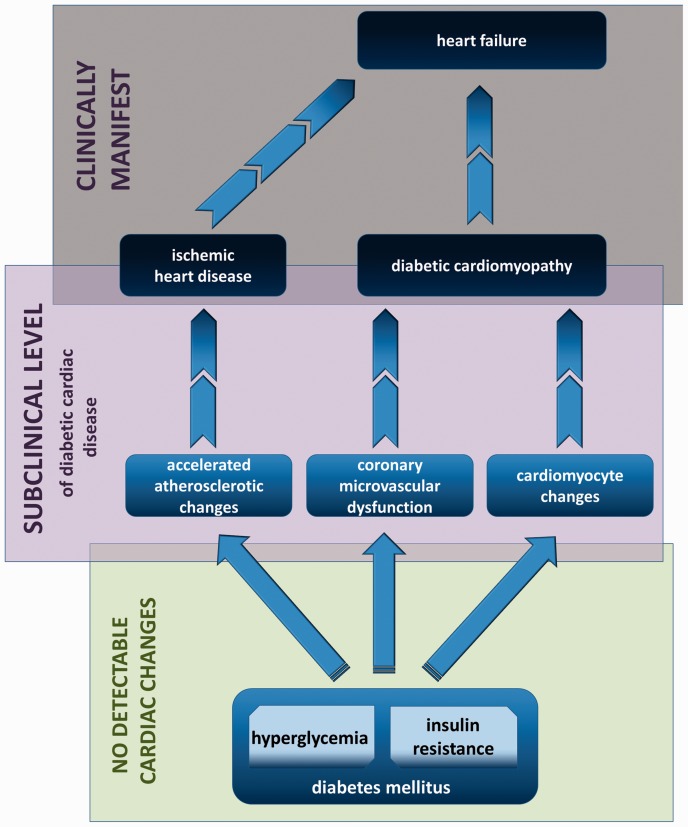
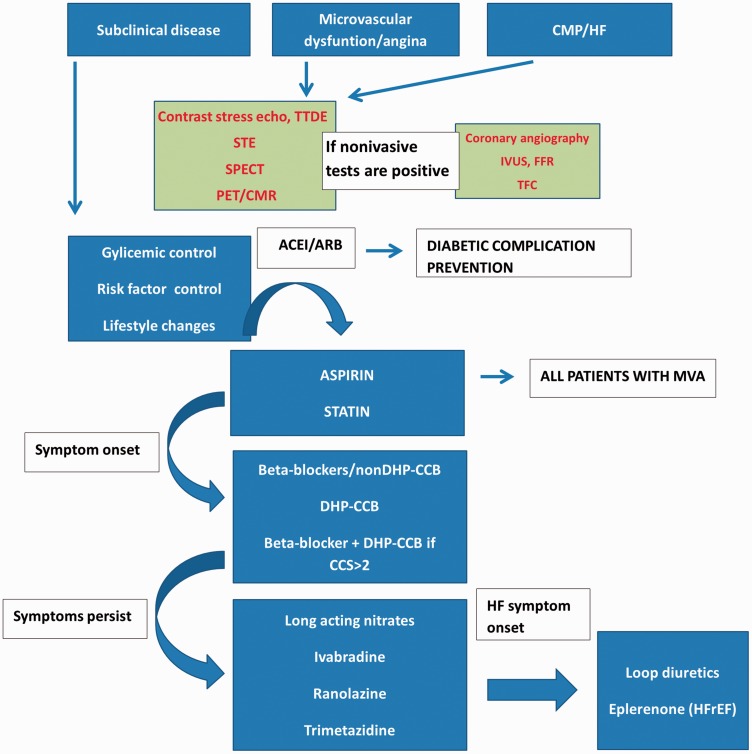
The significance, mechanisms and consequences of coronary microvascular dysfunction associated with diabetes mellitus are topics into which we have insufficient insight at this time. It is widely recognized that endothelial dysfunction that is caused by diabetes in various vascular beds contributes to a wide range of complications and exerts unfavorable effects on microcirculatory regulation. The coronary microcirculation is precisely regulated through a number of interconnected physiological processes with the purpose of matching local blood flow to myocardial metabolic demands. Dysregulation of this network might contribute to varying degrees of pathological consequences. This review discusses the most important findings regarding coronary microvascular dysfunction in diabetes from pre-clinical and clinical perspectives.
Keywords: Diabetes mellitus; arachidonic acid metabolites; artery; cardiomyopathy; coronary microvascular dysfunction; endothelial dysfunction; microcirculation; nitric oxide.
Figures
References
-
- Tousoulis D, Papageorgiou N, Androulakis E, et al. Diabetes mellitus-associated vascular impairment: novel circulating biomarkers and therapeutic approaches. J Am Coll Cardiol 2013; 62: 667–676. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
