

Repetitive peripheral magnetic stimulation for activities of daily living and functional ability in people after stroke
- PMID: 28644548
- PMCID: PMC6481821
- DOI: 10.1002/14651858.CD011968.pub2
Repetitive peripheral magnetic stimulation for activities of daily living and functional ability in people after stroke
Update in
-
Repetitive peripheral magnetic stimulation for impairment and disability in people after stroke.Cochrane Database Syst Rev. 2019 Nov 30;11(11):CD011968. doi: 10.1002/14651858.CD011968.pub3. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2022 Sep 28;9:CD011968. doi: 10.1002/14651858.CD011968.pub4. PMID: 31784991 Free PMC article. Updated.
Abstract
Background: Repetitive peripheral magnetic stimulation (rPMS) is a form of therapy that creates painless stimulation of deep muscle structures to improve motor function in people with physical impairment from brain or nerve disorders. Use of rPMS for people after stroke has been identified as a feasible approach to improve activities of daily living and functional ability. However, no systematic reviews have assessed the findings of available trials. The effect and safety of this intervention for people after stroke currently remain uncertain.
Objectives: To assess the effect of rPMS for improving activities of daily living and functional ability in people after stroke.
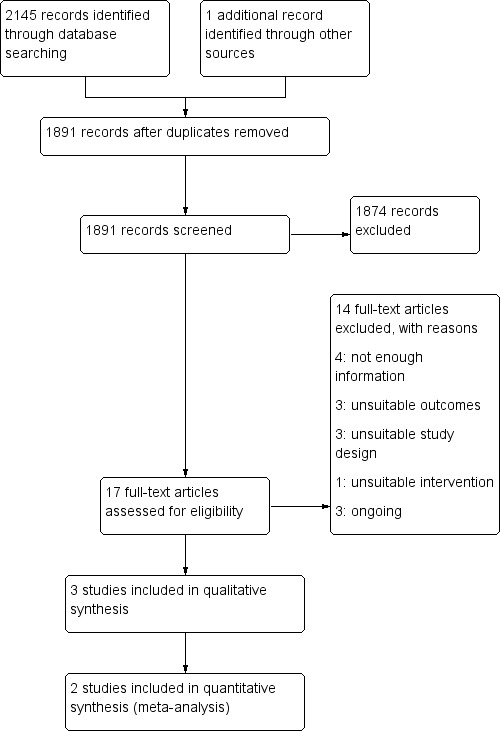
Search methods: We searched the Cochrane Stroke Group Trials Register (August 2016), the Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 8) in the Cochrane Library (August 2016), MEDLINE Ovid (November 2016), Embase Ovid (August 2016), the Cumulative Index to Nursing and Allied Health Literature (CINAHL) in Ebsco (August 2016), PsycINFO Ovid (August 2016), the Allied and Complementary Medicine Database (AMED) Ovid (August 2016), Occupational Therapy Systematic Evaluation of Evidence (OTseeker) (August 2016), the Physiotherapy Evidence Database (PEDro) (October 2016), and ICHUSHI Web (October 2016). We also searched five ongoing trial registries, screened reference lists, and contacted experts in the field. We placed no restrictions on the language or date of publication when searching the electronic databases.
Selection criteria: We included randomised controlled trials (RCTs) conducted to assess the therapeutic effect of rPMS for people after stroke. Comparisons eligible for inclusion were (1) active rPMS only compared with 'sham' rPMS (a very weak form of stimulation or a sound only); (2) active rPMS only compared with no intervention; (3) active rPMS plus rehabilitation compared with sham rPMS plus rehabilitation; and (4) active rPMS plus rehabilitation compared with rehabilitation only.
Data collection and analysis: Two review authors independently assessed studies for inclusion. The same review authors assessed methods and risk of bias and extracted data. We contacted trial authors to ask for unpublished information if necessary. We resolved all disagreements through discussion.
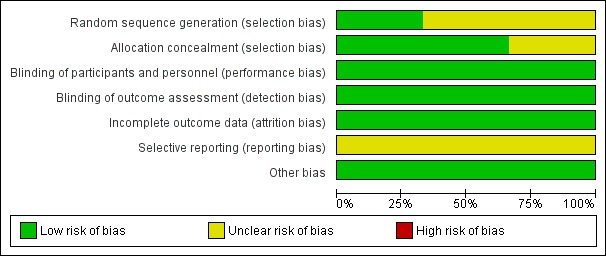
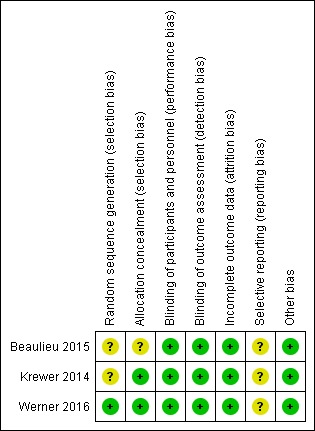
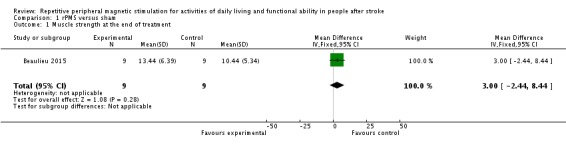
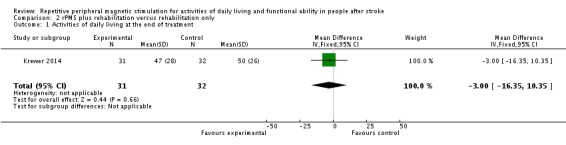
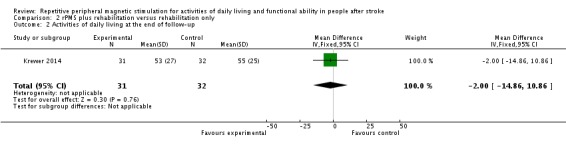
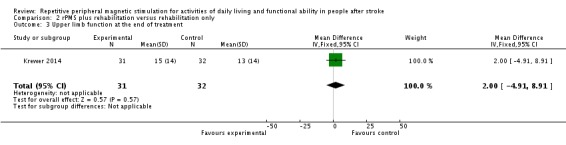
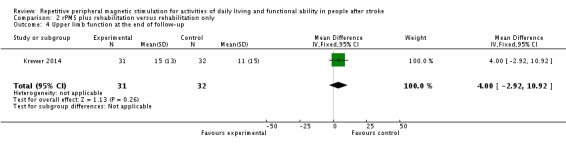
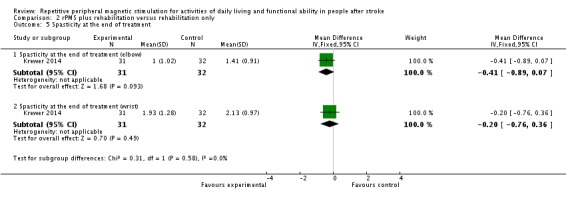
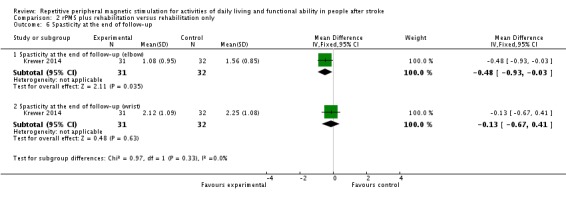
Main results: We included three trials (two RCTs and one cross-over trial) involving 121 participants. Blinding of participants and physicians was well reported in all trials, and overall risk of bias was low. We found no clear effect of rPMS on activities of daily living at the end of treatment (mean difference (MD) -3.00, 95% confidence interval (CI) -16.35 to 10.35; low-quality evidence) and at the end of follow-up (MD -2.00, 95% CI -14.86 to 10.86; low-quality evidence). Investigators in one study with 63 participants observed no statistical difference in improvement of upper limb function at the end of treatment (MD 2.00, 95% CI -4.91 to 8.91) and at the end of follow-up (MD 4.00, 95% CI -2.92 to 10.92). One trial with 18 participants showed that rPMS treatment was not associated with improved muscle strength at the end of treatment (MD 3.00, 95% CI -2.44 to 8.44). Another study reported a significant decrease in spasticity of the elbow at the end of follow-up (MD -0.48, 95% CI -0.93 to -0.03). No studies provided information on lower limb function and death. Based on the GRADE approach, we judged the certainty of evidence related to the primary outcome as low owing to the small sample size of one study.
Authors' conclusions: Available trials provided inadequate evidence to permit any conclusions about routine use of rPMS for people after stroke. Additional trials with large sample sizes are needed to determine an appropriate rPMS protocol as well as long-term effects. We identified three ongoing trials and will include these trials in the next review update.
Conflict of interest statement
Ryo Momosaki: none known. Naoki Yamada: none known. Erika Ota: none known. Masahiro Abo: none known.
Figures
References
References to studies included in this review
-
- Beaulieu L‐D, Masse‐Alarie H, Brouwer B, Schneider C. Noninvasive neurostimulation in chronic stroke: a double‐blind randomized sham‐controlled testing of clinical and corticomotor effects. Topics in Stroke Rehabilitation 2015;22(1):8‐17. - PubMed
-
- Krewer C, Hartl S, Muller F, Koenig E. Effects of repetitive peripheral magnetic stimulation on upper‐limb spasticity and impairment in patients with spastic hemiparesis: a randomized, double‐blind, sham‐controlled study. Archives of Physical Medicine and Rehabilitation 2014;95(6):1039‐47. - PubMed
-
- Werner C, Schrader M. Repetitive peripheral magnetic stimulation (rpMS) in combination with muscle stretch decreased the wrist and finger flexor muscle spasticity in chronic patients after CNS lesion. International Journal of Physical Medicine & Rehabilitation 2016;4:4.
References to studies excluded from this review
-
- Bernhardt M, Angerer B, Buss M, Struppler A. Isometric muscle contraction induced by repetitive peripheral magnetic stimulation (RPMS)‐modeling and identification. Biomedical Signal Processing and Control 2007;2(3):180‐90.
-
- Heldmann B, Kerkhoff G, Struppler A, Havel P, Jahn T. Repetitive peripheral magnetic stimulation alleviates tactile extinction. NeuroReport 2000;11(14):3193‐8. - PubMed
-
- Kuznetsova S, Kuznetsov V, Skachkova N. Enhancement of cortical excitability and motor function in stroke patients after combined repetitive transcranial and peripheral magnetic stimulation. European Journal of Neurology 2016;23:223. - PubMed
-
- Momosaki R, Abo M, Watanabe S, Kakuda W, Yamada N, Mochio K. Functional magnetic stimulation using a parabolic coil for dysphagia after stroke. Neuromodulation 2014;17(7):637‐641. - PubMed
-
- Rossini PM, Johnston CS. Facilitating acute stroke recovery with magnetic fields?. Neurology 2005;65(3):353‐4. - PubMed
References to studies awaiting assessment
-
- Kotchetkov A Gorbunov F, Streltsova N, Fillina T. Spasticity modulation using low frequency magnetic fields (LFMF) in stroke patients. 2nd World Congress in Neurological Rehabilitation 1999;42:42.
-
- Kuznetsova S, Kuznetsov V, Skachkova N. Combined central and peripheral magnetic stimulation to facilitate motor recovery after stroke. Cerebrovascular Diseases 2013;35 Suppl 3:548.
-
- Samosiuk NI. Magnetic and laser therapy of acute ischemic stroke. Voprosy Kurortologii, Fizioterapii, i Lechebnoi Fizicheskoi Kultury 2003;2:19‐20. - PubMed
-
- Zifko U, Morph M, Diem K, Havel P, Struppler A. Repetitive peripheral magnetic stimulation is effective in the rehabilitation of the paretic arm. Neurorehabilitation and Neural Repair 2002;16(1):18‐9.
References to ongoing studies
-
- Effect of pairing peripheral and transcranial magnetic stimulations triggered by actual movement on motor plasticity. UMIN‐CTR (accessed August 2016). [UMIN000019106]
-
- The effect of repetitive peripheral magnetic stimulation in stroke‐rehabilitation: a randomized controlled trial. German Clinical Trials Register (accessed August 2016). [DRKS00007722]
-
- The effects of repetitive peripheral magnetic stimulation in patient with spastic hemiparesis after stroke: a randomized‐controlled study. German Clinical Trials Register (accessed August 2016). [DRKS00007899]
-
- Repetitive peripheral magnetic stimulation for patients with hemiplegia. UMIN‐CTR (accessed August 2016). [UMIN000018750]
Additional references
-
- Barker AT. An introduction to the basic principles of magnetic nerve stimulation. Journal of Clinical Neurophysiology 1991;8:26‐37. - PubMed
-
- Beaulieu LD, Schneider C. Effects of repetitive peripheral magnetic stimulation on normal or impaired motor control. A review. Clinical Neurophysiology 2013;43(4):251‐60. - PubMed
-
- Beaulieu LD, Schneider C. Repetitive peripheral magnetic stimulation to reduce pain or improve sensorimotor impairments: a literature review on parameters of application and afferents recruitment. Neurophysiologie Clinique 2015;45(3):223‐37. - PubMed
-
- Melbourne, Australia: Veritas Health Innovation. Covidence systematic review software. Melbourne, Australia: Veritas Health Innovation, 2013.
-
- Vries S, Mulder T. Motor imagery and stroke rehabilitation: a critical discussion. Journal of Rehabilitation Medicine 2007;39(1):5‐13. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical