

Patient-experienced burden of treatment in patients with multimorbidity - A systematic review of qualitative data
- PMID: 28644877
- PMCID: PMC5482482
- DOI: 10.1371/journal.pone.0179916
Patient-experienced burden of treatment in patients with multimorbidity - A systematic review of qualitative data
Abstract
Objective: To synthesize existing qualitative literature on patient-experienced burden of treatment in multimorbid patients.
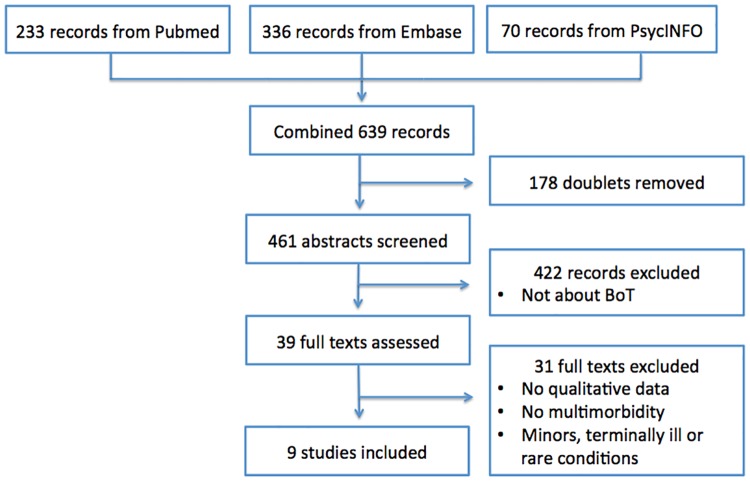
Methods: A literature search identified available qualitative studies on the topic of burden of treatment in multimorbidity and meta-ethnography was applied as method. The authors' original findings were preserved, but also synthesized to new interpretations to investigate the concept of the burden of treatment using the Cumulative Complexity Model.
Results: Nine qualitative studies were identified. The majority of the 1367 participants from 34 different countries were multimorbid. The treatment burden components, experienced by patients, were identified for each study. The components financial burden, lack of knowledge, diet and exercise, medication burden and frequent healthcare reminding patients of their health problem were found to attract additional attention from the multimorbid patients. In studies conducted in the US and Australia the financial burden and the time and travel burden were found most straining to patients with deprived socioeconomic status. The burden of treatment was found to be a complex concept consisting of many different components and factors interacting with each other. The size of the burden was associated to the workload of demands (number of conditions, number of medications and health status), the capacity (cognitive, physical and financial resources, educational level, cultural background, age, gender and employment conditions) and the context (structure of healthcare and social support). Patients seem to use strategies such as prioritizing between treatments to diminish the workload and mobilizing and coordinating resources to improve their ability to manage the burden of treatment. They try to routinize and integrate the treatment into their daily lives, which might be a way to maintain the balance between workload and capacity.
Conclusions: Healthcare providers need to increase the focus on minimizing multimorbid patients' burden of treatment. Findings in this review suggest that the weight of the burden needs to be established in the individual patient and components of the burden must be identified.
Conflict of interest statement
Figures
References
-
- Ward BW, Schiller JS, Goodman RA. Multiple chronic conditions among US adults: a 2012 update. Preventing chronic disease. 2014;11:E62 doi: 10.5888/pcd11.130389 ; - DOI - PMC - PubMed
-
- WHO USDoHaHSa. Global Health and Aging. 2011.
-
- Willadsen TG, Bebe A, Koster-Rasmussen R, Jarbol DE, Guassora AD, Waldorff FB, et al. The role of diseases, risk factors and symptoms in the definition of multimorbidity—a systematic review. Scandinavian journal of primary health care. 2016;34(2):112–21. doi: 10.3109/02813432.2016.1153242 ; - DOI - PMC - PubMed
-
- Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PloS one. 2014;9(7):e102149 doi: 10.1371/journal.pone.0102149 ; - DOI - PMC - PubMed
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi: 10.1016/S0140-6736(12)60240-2 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
