

Percutaneous Treatment of Unstable Scaphoid Waist Fractures
- PMID: 28644940
- PMCID: PMC5484455
- DOI: 10.1177/1558944716681948
Percutaneous Treatment of Unstable Scaphoid Waist Fractures
Abstract
Background: Percutaneous techniques have been described for the treatment of nondisplaced scaphoid fractures, although less information has been reported about outcomes for unstable, displaced fractures. The aim of this study was to evaluate the union and complication rates following manual closed reduction and percutaneous screw placement for a consecutive series of unstable, displaced scaphoid fractures.
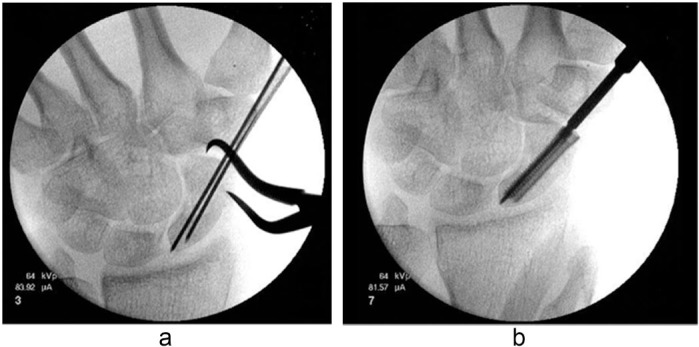
Methods: A total of 28 patients (average age, 27 years; 22 male/6 female) were treated for isolated unstable displaced scaphoid waist fractures. Closed reduction and percutaneous headless, compression screw fixation was successfully performed in 14 patients (average age, 32 years; 10 male/4 female), and the remaining 14 patients required open reduction. Patients who underwent percutaneous treatment were followed for radiographic fracture union and clinical outcomes.
Results: Thirteen of 14 fractures (93%) had clinical and radiographic evidence of bone union at an average of 2.8 months postoperatively. Average visual analog pain score at the time of union was 0.9. The average Quick Disability of the Arm, Shoulder, and Hand score at 2.5 years follow-up (range, 1.5-8.3 years) was 9.6 (range, 0.0-27.3). Complications included 1 case of nonunion and 1 case of intraoperative Kirschner wire breakage.
Conclusions: Manual closed reduction followed by percutaneous headless, compression screw fixation was possible in 50% of patients who presented with acute unstable, displaced scaphoid fractures. This technique appears to be a safe and effective method when a manual reduction is possible, and it may offer a less invasive option when compared with a standard open technique.
Keywords: fracture; navicular; percutaneous; scaphoid; unstable.
Conflict of interest statement
Figures


References
-
- Adolfsson L, Lindau T, Arner M. Acutrak screw fixation versus cast immobilisation for undisplaced scaphoid waist fractures. J Hand Surg Br. 2001;26(3):192-195. - PubMed
-
- Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP, III, Linscheid RL. Scaphoid malunion. J Hand Surg Am. 1989;14(4):679-687. - PubMed
-
- Arora R, Gschwentner M, Krappinger D, Lutz M, Blauth M, Gabl M. Fixation of nondisplaced scaphoid fractures: making treatment cost effective. Arch Orthop Trauma Surg. 2007;127(1):39-46. - PubMed
-
- Beaton DE, Wright JG, Katz JN. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005;87(5):1038-1046. - PubMed
-
- Bedi A, Jebson PJ, Hayden RJ, Jacobson JA, Martus JE. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am. 2007;32(3):326-333. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
