

Analgosedation Practices and the Impact of Sedation Depth on Clinical Outcomes Among Patients Requiring Mechanical Ventilation in the ED: A Cohort Study
- PMID: 28645462
- PMCID: PMC5812748
- DOI: 10.1016/j.chest.2017.05.041
Analgosedation Practices and the Impact of Sedation Depth on Clinical Outcomes Among Patients Requiring Mechanical Ventilation in the ED: A Cohort Study
Abstract
Background: Analgesia and sedation are cornerstone therapies for mechanically ventilated patients. Despite data showing that early deep sedation in the ICU influences outcome, this has not been investigated in the ED. Therefore, ED-based sedation practices, and their influence on outcome, remain incompletely defined. This study's objectives were to describe ED sedation practices in mechanically ventilated patients and to test the hypothesis that ED sedation depth is associated with worse outcomes.
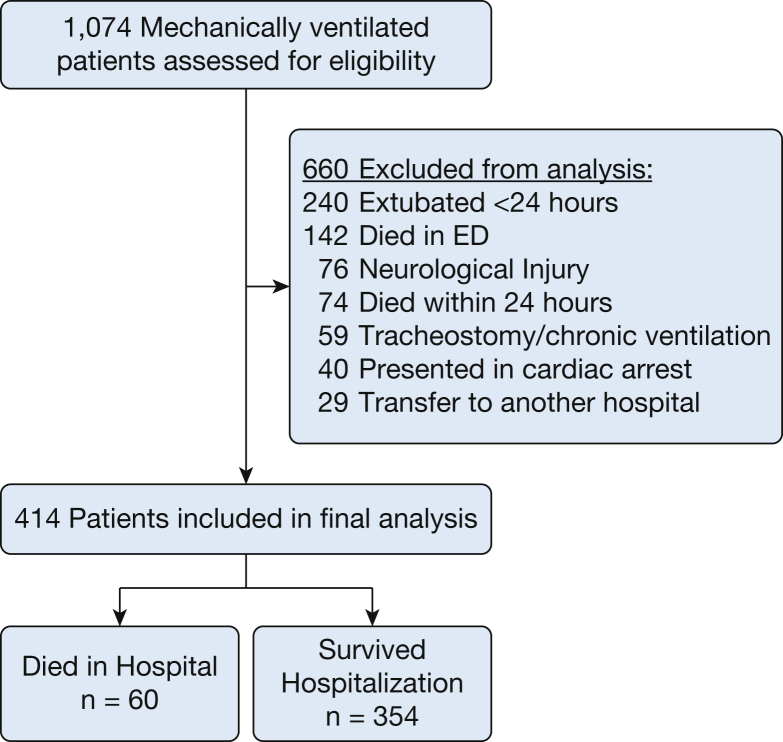
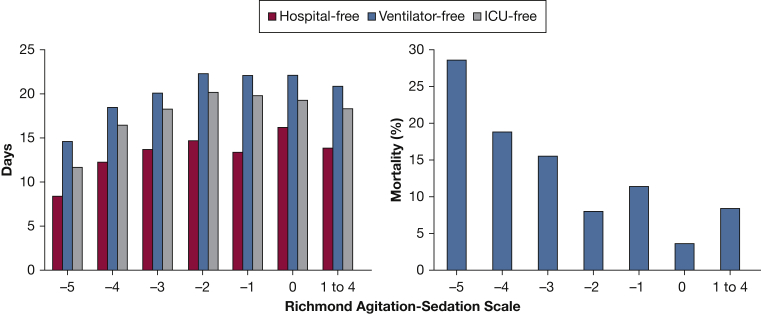
Methods: This was a cohort study of a prospectively compiled ED registry of adult mechanically ventilated patients at a single academic medical center. Hospital mortality was the primary outcome and hospital-, ICU-, and ventilator-free days were secondary outcomes. A backward stepwise multivariable logistic regression model evaluated the primary outcome as a function of ED sedation depth. Sedation depth was assessed with the Richmond Agitation-Sedation Scale (RASS).
Results: Four hundred fourteen patients were studied. In the ED, 354 patients (85.5%) received fentanyl, 254 (61.3%) received midazolam, and 194 (46.9%) received propofol. Deep sedation was observed in 244 patients (64.0%). After adjusting for confounders, a deeper ED RASS was associated with mortality (adjusted OR, 0.77; 95% CI, 0.63-0.94).
Conclusions: Early deep sedation is common in mechanically ventilated ED patients and is associated with worse mortality. These data suggest that ED-based sedation is a modifiable variable that could be targeted to improve outcome.
Keywords: ED; mechanical ventilation; sedation depth.
Copyright © 2017 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Barr J., Fraser G.L., Puntillo K. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. - PubMed
-
- Bonomo J.B., Butler A.S., Lindsell C.J., Venkat A. Inadequate provision of postintubation anxiolysis and analgesia in the ED. Am J. Emerg Med. 2008;26(4):469–472. - PubMed
-
- Chong I.D., Sandefur B.J., Rimmelin D.E. Long-acting neuromuscular paralysis without concurrent sedation in emergency care. Am J Emerg Med. 2014;32(5):452–456. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
