

Stereotactic radiosurgery versus whole-brain radiotherapy after intracranial metastasis resection: a systematic review and meta-analysis
- PMID: 28646895
- PMCID: PMC5483276
- DOI: 10.1186/s13014-017-0840-x
Stereotactic radiosurgery versus whole-brain radiotherapy after intracranial metastasis resection: a systematic review and meta-analysis
Abstract
Background: In patients with one to three brain metastases who undergo resection, options for post-operative treatments include whole-brain radiotherapy (WBRT) or stereotactic radiosurgery (SRS) of the resection cavity. In this meta-analysis, we sought to compare the efficacy of each post-operative radiation modality with respect to tumor recurrence and survival.
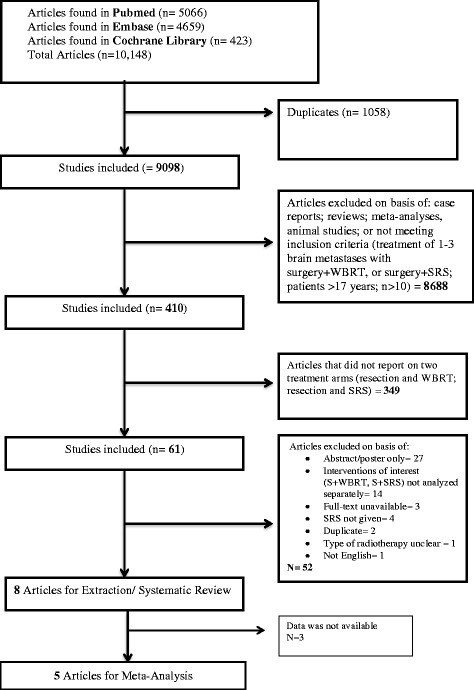
Methods: Pubmed, Embase and Cochrane databases were searched through June 2016 for cohort studies reporting outcomes of SRS or WBRT after metastasis resection. Pooled effect estimates were calculated using fixed-effect and random-effect models for local recurrence, distant recurrence, and overall survival.
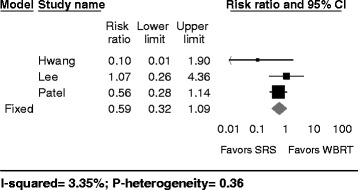
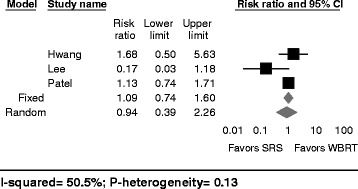
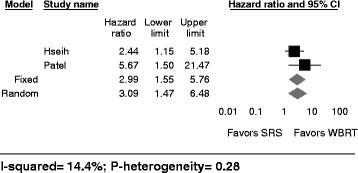
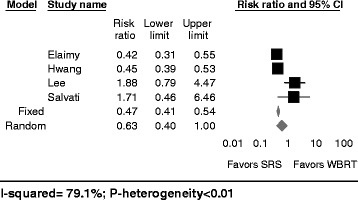
Results: Eight retrospective cohort studies with 646 patients (238 with SRS versus 408 with WBRT) were included in the analysis. Comparing SRS to WBRT, the overall crude risk ratio using the fixed-effect model was 0.59 for local recurrence (95%-CI: 0.32-1.09, I2: 3.35%, P-heterogeneity = 0.36, 3 studies), 1.09 for distant recurrence (95%-CI: 0.74-1.60, I2: 50.5%, P-heterogeneity = 0.13; 3 studies), and 2.99 for leptomeningeal disease (95% CI 1.55-5.76; I2: 14.4% p-heterogeneity: 0.28; 2 studies). For the same comparison, the risk ratio for median overall survival was 0.47 (95% CI: 0.41-0.54; I2: 79.1%, P-heterogeneity < 0.01; 4 studies) in a fixed-effect model, but was no longer significant (0.63; 95%-CI: 0.40-1.00) in a random-effect model. SRS was associated with a lower risk of leukoencephalopathy (RR: 0.15, 95% CI: 0.07-0.33, 1 study), yet with a higher risk of radiation-necrosis (RR: 19.4, 95% CI: 1.21-310, 1 study).
Conclusion: Based on retrospective cohort studies, the results of this study suggest that SRS of the resection cavity may offer comparable survival and similar local and distant control as adjuvant WBRT, yet may be associated with a higher risk for developing leptomeningeal disease. Future research on SRS should focus on achieving a better understanding of the various factors that may favor SRS over WBRT.
Keywords: Brain Metastasis; Meta-analysis; Resection; Stereotactic radiosurgery; Whole brain radiation.
Figures
References
-
- Iorio-Morin C, Masson-Cote L, Ezahr Y, Blanchard J, Ebacher A, Mathieu D. Early Gamma Knife stereotactic radiosurgery to the tumor bed of resected brain metastasis for improved local control. J Neurosurg. 2014;121(Suppl):69–74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
