

Outcomes of Preterm Infants following Discussions about Withdrawal or Withholding of Life Support
- PMID: 28647272
- PMCID: PMC5690862
- DOI: 10.1016/j.jpeds.2017.05.056
Outcomes of Preterm Infants following Discussions about Withdrawal or Withholding of Life Support
Erratum in
-
Corrigendum to 'Outcomes of Preterm Infants following Discussions about Withdrawal or Withholding of Life Support'.J Pediatr. 2019 Apr;207:270. doi: 10.1016/j.jpeds.2018.09.006. J Pediatr. 2019. PMID: 30922501 No abstract available.
Abstract
Objectives: To describe the frequency of postnatal discussions about withdrawal or withholding of life-sustaining therapy (WWLST), ensuing WWLST, and outcomes of infants surviving such discussions. We hypothesized that such survivors have poor outcomes.
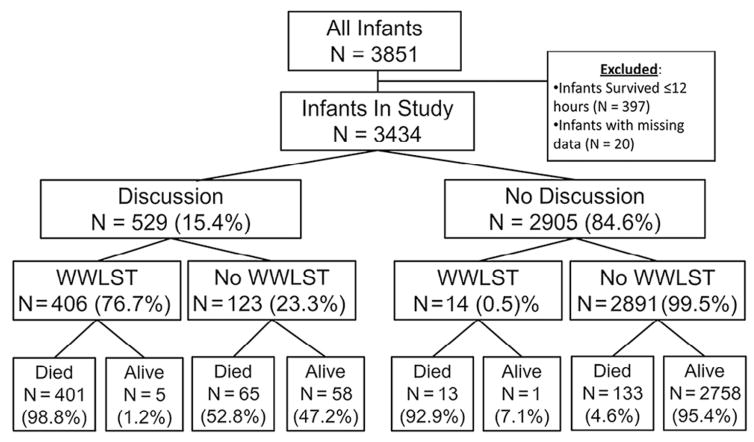
Study design: This retrospective review included registry data from 18 centers of the National Institute of Child Health and Human Development Neonatal Research Network. Infants born at 22-28 weeks of gestation who survived >12 hours during 2011-2013 were included. Regression analysis identified maternal and infant factors associated with WWLST discussions and factors predicting ensuing WWLST. In-hospital and 18- to 26-month outcomes were evaluated.
Results: WWLST discussions occurred in 529 (15.4%) of 3434 infants. These were more frequent at 22-24 weeks (27.0%) compared with 27-28 weeks of gestation (5.6%). Factors associated with WWLST discussion were male sex, gestational age (GA) of ≤24 weeks, birth weight small for GA, congenital malformations or syndromes, early onset sepsis, severe brain injury, and necrotizing enterocolitis. Rates of WWLST discussion varied by center (6.4%-29.9%) as did WWLST (5.2%-20.7%). Ensuing WWLST occurred in 406 patients; of these, 5 survived to discharge. Of the 123 infants for whom intensive care was continued, 58 (47%) survived to discharge. Survival after WWLST discussion was associated with higher rates of neonatal morbidities and neurodevelopmental impairment compared with babies for whom WWLST discussions did not occur. Significant predictors of ensuing WWLST were maternal age >25 years, necrotizing enterocolitis, and days on a ventilator.
Conclusions: Wide center variations in WWLST discussions occur, especially at ≤24 weeks GA. Outcomes of infants surviving after WWLST discussions are poor.
Trial registration: ClinicalTrials.gov: NCT00063063.
Keywords: disability; ethics; newborn; palliative care; prognosis.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Comment in
-
Threading the Needle for the Tiniest Babies.J Pediatr. 2017 Nov;190:8-9. doi: 10.1016/j.jpeds.2017.07.030. J Pediatr. 2017. PMID: 29144276 No abstract available.
References
-
- Weiner J, Sharma J, Lantos J, Kilbride H. How infants die in the neonatal intensive care unit: trends from 1999 through 2008. Arch Pediatr Adolesc Med. 2011;165:630–4. - PubMed
-
- Barton L, Hodgman JE. The contribution of withholding or withdrawing care to newborn mortality. Pediatrics. 2005;116:1487–91. - PubMed
-
- Singh J, Lantos J, Meadow W. End-of-life after birth: death and dying in a neonatal intensive care unit. Pediatrics. 2004;114:1620–6. - PubMed
-
- Aladangady N, Shaw C, Gallagher K, Stokoe E, Marlow N for Collaborators Group. Short-term outcome of treatment limitation discussions for newborn infants, a multicentre prospective observational cohort study. Arch Dis Child Fetal Neonatal Ed. 2017;102:F104–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- UG1 HD068263/HD/NICHD NIH HHS/United States
- UL1 TR001111/TR/NCATS NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD068270/HD/NICHD NIH HHS/United States
- M01 RR000030/RR/NCRR NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD068244/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- UL1 TR000042/TR/NCATS NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- M01 RR000059/RR/NCRR NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD068244/HD/NICHD NIH HHS/United States
- U10 HD068263/HD/NICHD NIH HHS/United States
- M01 RR000633/RR/NCRR NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- U10 HD068270/HD/NICHD NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- M01 RR000032/RR/NCRR NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UL1 TR001117/TR/NCATS NIH HHS/United States
- U10 HD068284/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- U10 HD068278/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
