

Transitions From Skilled Nursing Facility to Home: The Relationship of Early Outpatient Care to Hospital Readmission
- PMID: 28647577
- PMCID: PMC5612845
- DOI: 10.1016/j.jamda.2017.05.007
Transitions From Skilled Nursing Facility to Home: The Relationship of Early Outpatient Care to Hospital Readmission
Abstract
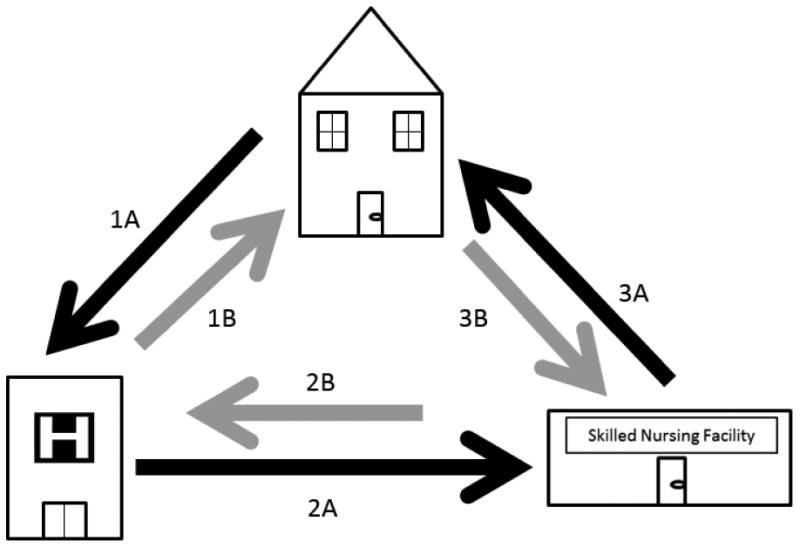
Background: Many adults are discharged to skilled nursing facilities (SNFs) prior to returning home from the hospital. Patient characteristics and factors that can help to prevent postdischarge adverse outcomes are poorly understood.
Objective: To identify whether early post-SNF discharge care reduces likelihood of 30-day hospital readmissions.
Design: Secondary data analysis using the Electronic Medical Record, Medicare, Medicaid and the Minimum Data Set.
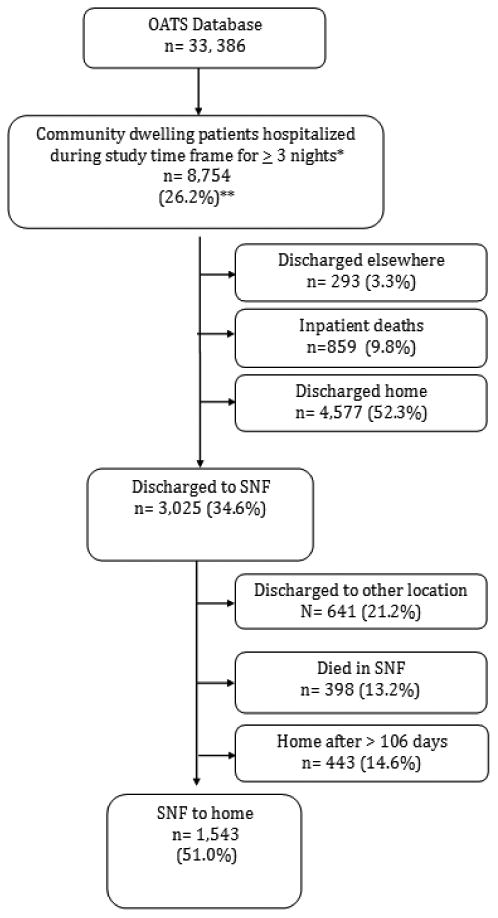
Participants/setting: Older (age > 65 years), community-dwelling adults admitted to a safety net hospital in the Midwest for 3 or more nights and discharged home after an SNF stay (n = 1543).
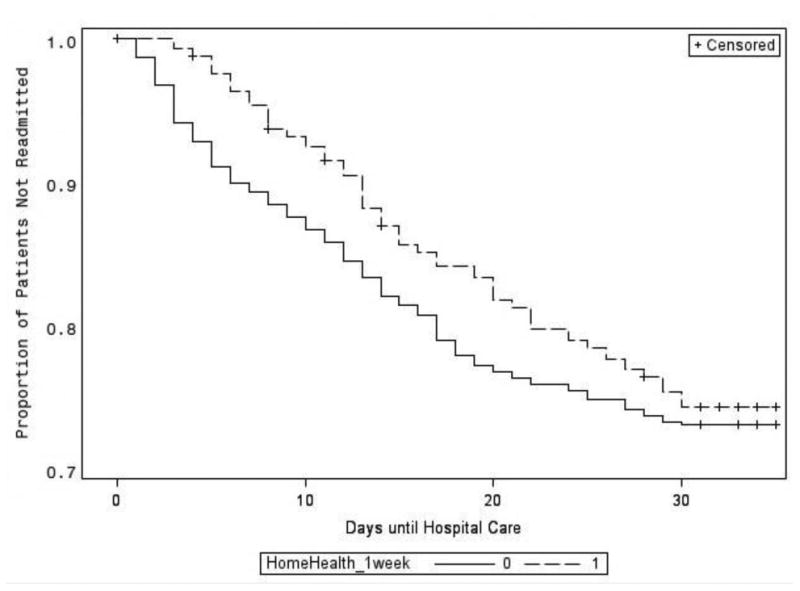
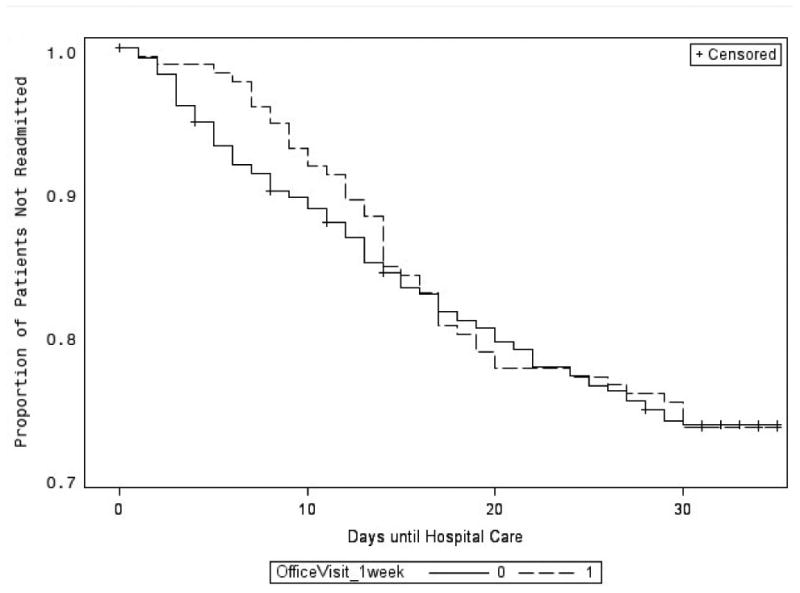
Measurements: The primary outcome was hospital readmission within 30 days of SNF discharge. The primary independent variables were either a home health visit or an outpatient provider visit within a week of SNF discharge.
Results: Out of 8754 community-dwelling, hospitalized older adults, 3025 (34.6%) were discharged to an SNF, of whom 1543 (51.0%) returned home. Among the SNF to home group, a home health visit within a week of SNF discharge was associated with reduced hazard of 30-day hospital readmission [adjusted hazard ratio (aHR) 0.61, P < .001] but outpatient provider visits were not associated with reduced risk of hospital readmission (aHR = 0.67, P = .821).
Conclusion: For patients discharged from an SNF to home, the finding that a home health visit within a week of discharge is associated with reduced hazard of 30-day hospital readmissions suggests a potential avenue for intervention.
Keywords: Care transitions; home care; hospital readmission; primary care; skilled nursing facility.
Copyright © 2017 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
No authors have conflicts of interest to report.
Figures
References
-
- Commission MPA. Data Book: Healthcare spending and the Medicare program. [Accessed June 1, 2016];2015 Jun; http://medpac.gov/documents/data-book/june-2015-databook-health-care-spe....
-
- David S, Sheikh F, Mahajan D, Greenough W, Bellantoni M. Whom Do We Serve? Describing the target population for post-acute and long-term care, focusing on nursing facility, settings, in the era of population health. 2016 http://www.paltc.org/amda-white-papers-and-resolution-position-statement.... - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
