

Acute Kidney Injury After Primary Angioplasty: Is Contrast-Induced Nephropathy the Culprit?
- PMID: 28647690
- PMCID: PMC5669180
- DOI: 10.1161/JAHA.117.005715
Acute Kidney Injury After Primary Angioplasty: Is Contrast-Induced Nephropathy the Culprit?
Abstract
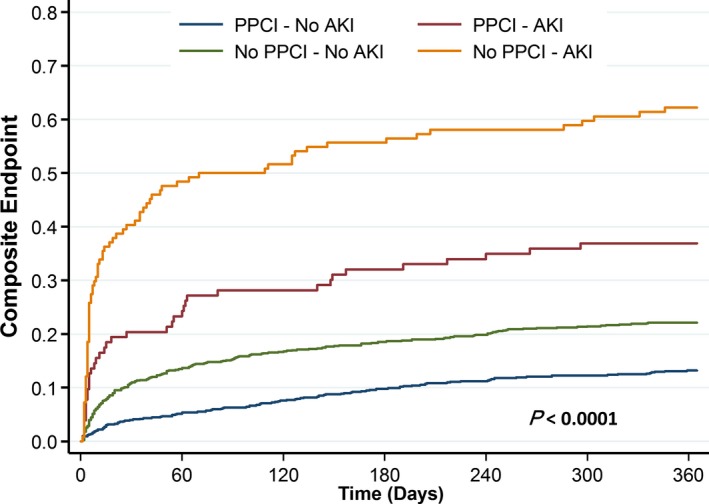
Background: Acute kidney injury (AKI) following primary percutaneous coronary intervention (pPCI) is frequently interpreted as contrast-induced AKI but may result from other insults. We aimed to determine the causal association of contrast material exposure and the incidence of AKI following pPCI using a control group of propensity score-matched patients with ST-segment-elevation myocardial infarction who were not exposed to contrast material.
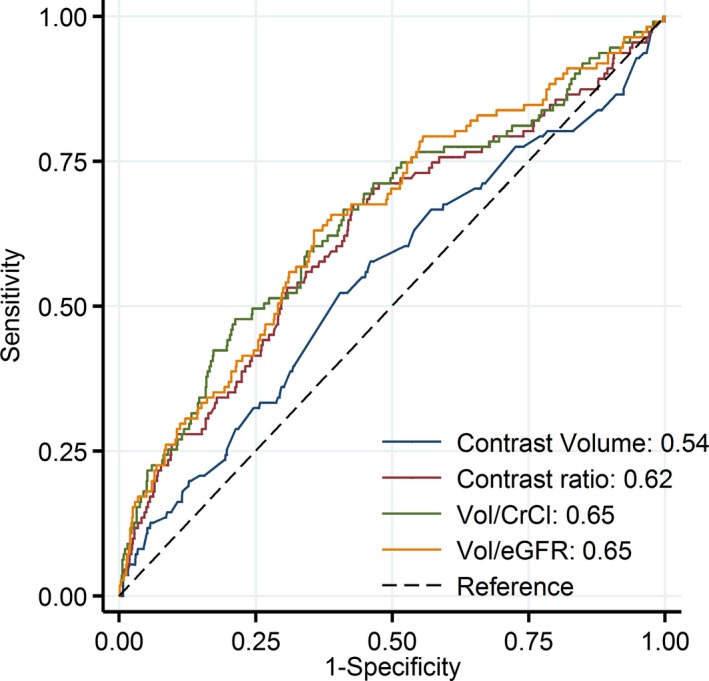
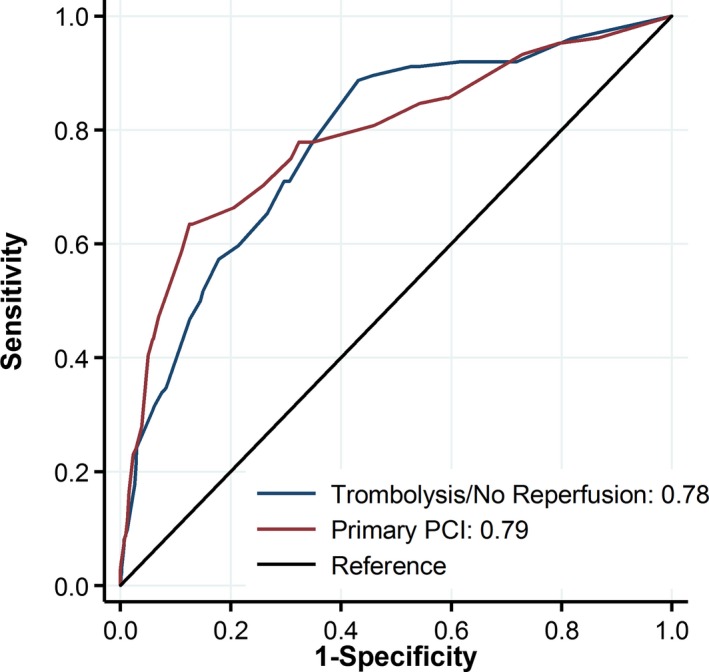
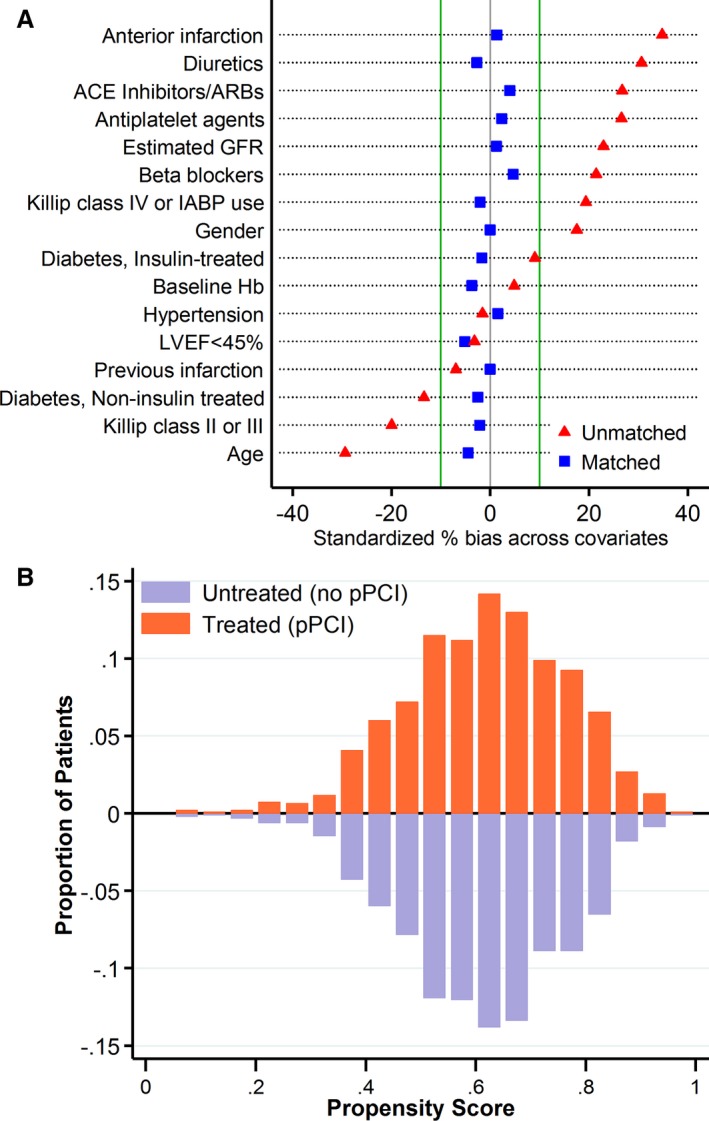
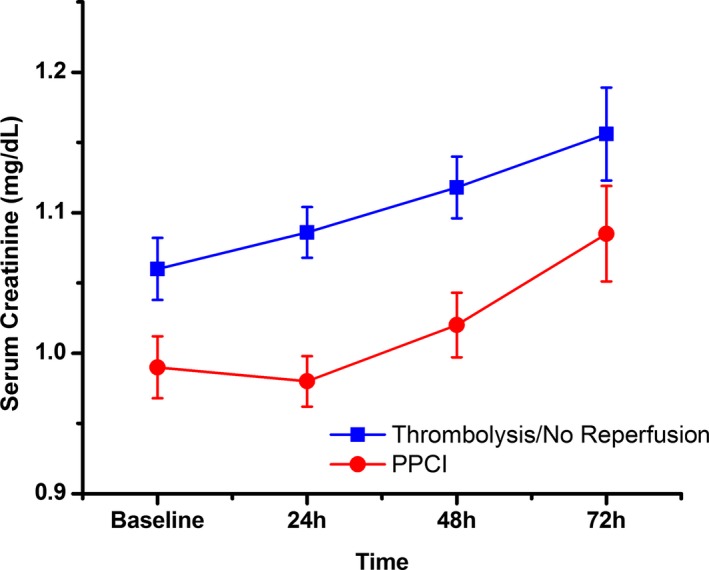
Methods and results: We studied 2025 patients with ST-segment-elevation myocardial infarction who underwent pPCI and 1025 patients receiving fibrinolysis or no reperfusion who were not exposed to contrast material during the first 72 hours of hospital stay (control group). AKI was defined as creatinine of ≥0.5 mg/dL or >25% rise within 72 hours. AKI rates were similar in the pPCI and control groups (10.3% versus 12.1%, respectively; P=0.38). Propensity score matching resulted in 931 matched pairs with PCI and no PCI, with balanced baseline covariates (standardized difference <0.1). Among propensity score-matched patients, AKI rates were not significantly different with and without PCI (8.6% versus 10.9%, P=0.12). In the pPCI cohort, independent predictors of AKI included age ≥70 years, insulin-treated diabetes mellitus, diuretic therapy, anterior infarction, baseline estimated glomerular filtration rate, and variables related to the presence of pump failure (higher Killip class, intra-aortic balloon pump use) and reduced left ventricular ejection fraction but not contrast material dose. A risk score based on the PCI cohort had similar discriminatory capacity for AKI in the control group (C statistic 0.81±0.02 and 0.78±0.02, respectively; P=0.26).
Conclusions: The development of AKI in patients with ST-segment-elevation myocardial infarction undergoing pPCI is mainly related to older age, baseline estimated glomerular filtration rate, heart failure, and hemodynamic instability. Risk for AKI is similar among ST-segment-elevation myocardial infarction patients with and without contrast material exposure.
Keywords: contrast media; contrast‐induced nephropathy; myocardial infarction; primary percutaneous coronary intervention.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Marenzi G, Lauri G, Assanelli E, Campodonico J, De Metrio M, Marana I, Grazi M, Veglia F, Bartorelli AL. Contrast‐induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol. 2004;44:1780–1785. - PubMed
-
- Marenzi G, Assanelli E, Campodonico J, Lauri G, Marana I, De Metrio M, Moltrasio M, Grazi M, Rubino M, Veglia F, Fabbiocchi F, Bartorelli AL. Contrast volume during primary percutaneous coronary intervention and subsequent contrast‐induced nephropathy and mortality. Ann Intern Med. 2009;150:170–177. - PubMed
-
- Narula A, Mehran R, Weisz G, Dangas GD, Yu J, Genereux P, Nikolsky E, Brener SJ, Witzenbichler B, Guagliumi G, Clark AE, Fahy M, Xu K, Brodie BR, Stone GW. Contrast‐induced acute kidney injury after primary percutaneous coronary intervention: results from the HORIZONS‐AMI substudy. Eur Heart J. 2014;35:1533–1540. - PubMed
-
- McCullough PA. Contrast‐induced acute kidney injury. J Am Coll Cardiol. 2008;51:1419–1428. - PubMed
-
- Morcos SK, Thomsen HS, Webb JA. Contrast‐media‐induced nephrotoxicity: a consensus report. Contrast Media Safety Committee, European Society of Urogenital Radiology (ESUR). Eur Radiol. 1999;9:1602–1613. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
