

Risk of ESRD and Mortality Associated With Change in Filtration Markers
- PMID: 28648303
- PMCID: PMC5610931
- DOI: 10.1053/j.ajkd.2017.04.025
Risk of ESRD and Mortality Associated With Change in Filtration Markers
Abstract
Background: Using change in estimated glomerular filtration rate (eGFR) based on creatinine concentration as a surrogate outcome in clinical trials of chronic kidney disease has been proposed. Risk for end-stage renal disease (ESRD) and all-cause mortality associated with change in concentrations of other filtration markers has not been studied in chronic kidney disease populations.
Study design: Observational analysis of 2 clinical trials.
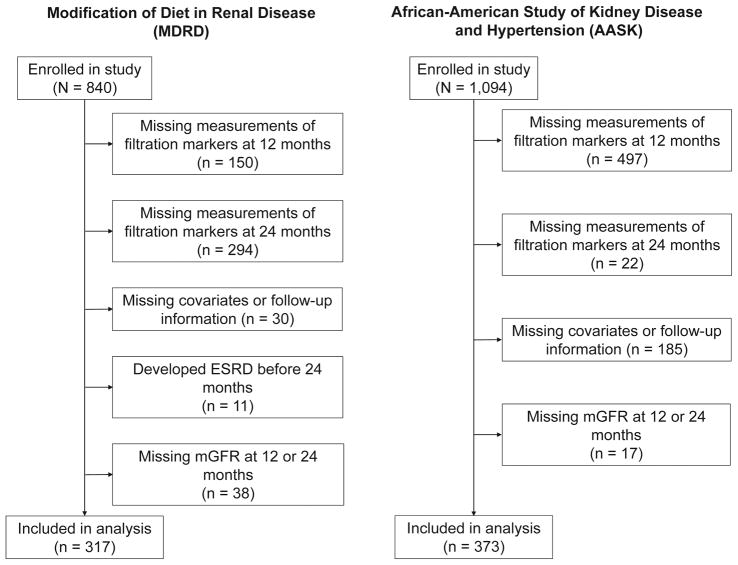
Setting & participants: Participants in the MDRD (Modification of Diet in Renal Disease; n=317) Study and AASK (African American Study of Kidney Disease and Hypertension; n=373).
Predictors: Creatinine, cystatin C, β-trace protein (BTP), and β2-microglobulin (B2M) were measured in serum samples collected at the 12- and 24-month follow-up visits, along with measured GFR (mGFR) at these time points.
Outcomes: ESRD and all-cause mortality.
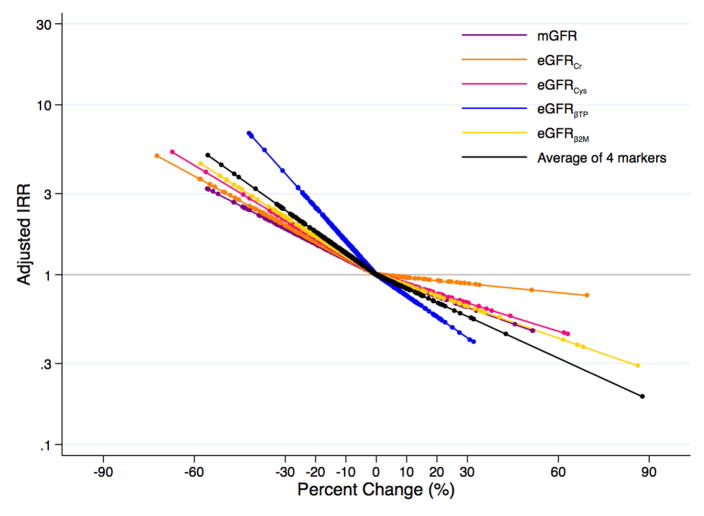
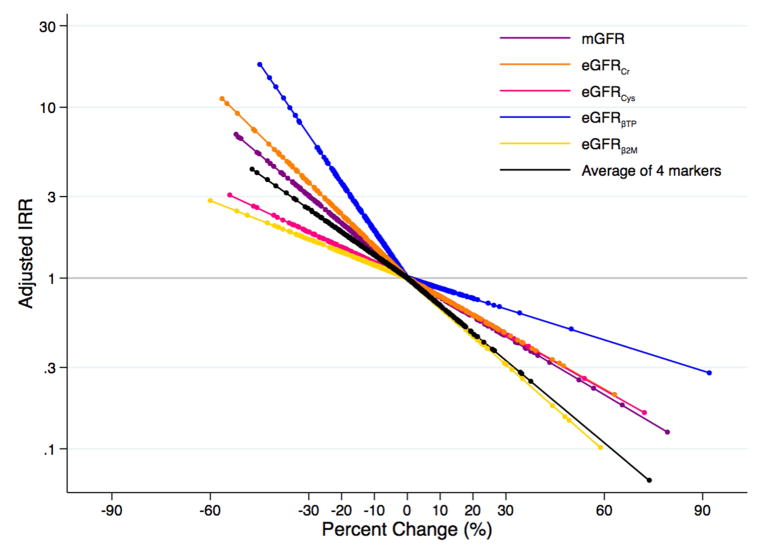
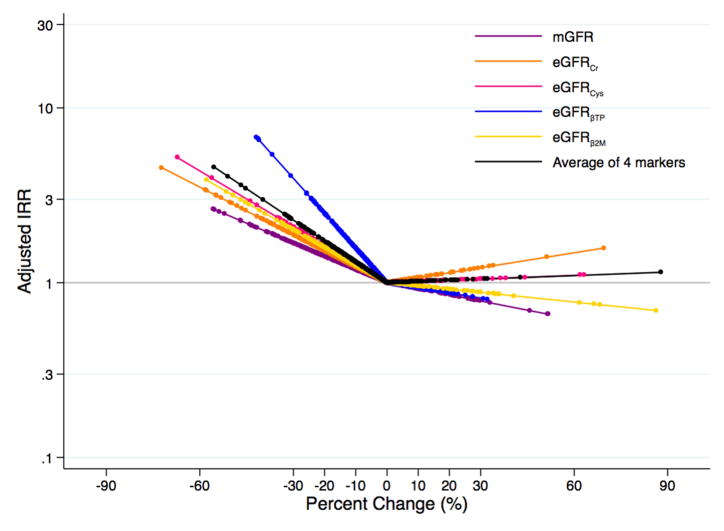
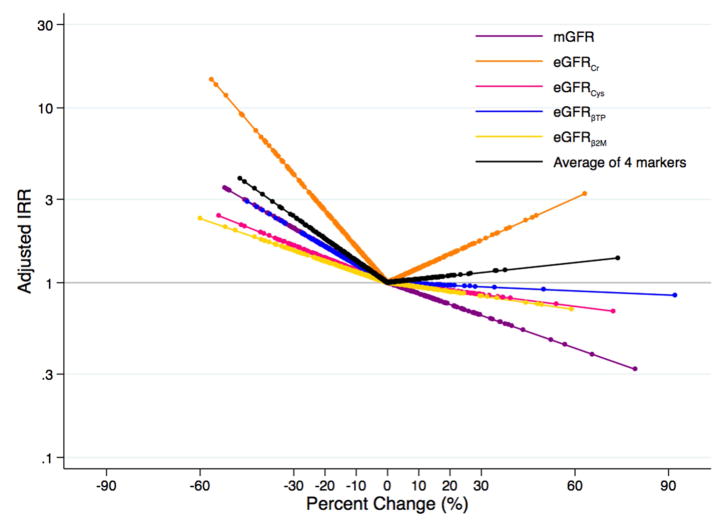
Measurements: Poisson regression was used to estimate incidence rate ratios and 95% CIs for ESRD and all-cause mortality during long-term follow-up (10-16 years) per 30% decline in mGFR or eGFR for each filtration marker and the average of all 4 markers.
Results: 1-year decline in mGFR, eGFRcr, eGFRBTP, and the average of the 4 filtration markers was significantly associated with increased risk for incident ESRD in both studies (all P≤0.02). Compared to mGFR, only decline in eGFRBTP was statistically significantly more strongly associated with ESRD risk in both studies (both P≤0.03). Decline in eGFRcr, but not mGFR or the other filtration markers, was significantly associated with risk for all-cause mortality in AASK only (incidence rate ratio per 30% decline, 4.17; 95% CI, 1.78-9.74; P<0.001), but this association was not significantly different from decline in mGFR (P=0.2).
Limitations: Small sample size.
Conclusions: Declines in mGFR, eGFRcr, eGFRBTP, and the average of 4 filtration markers (creatinine, cystatin C, BTP, and B2M) were consistently associated with progression to ESRD.
Keywords: Beta-2-microglobulin (B2M); beta trace protein (BTP); creatinine; cystatin C; death; end-stage renal disease (ESRD); estimated GFR; filtration markers; glomerular filtration rate (GFR); incident ESRD; kidney function decline; measured GFR; mortality.
Copyright © 2017 National Kidney Foundation, Inc. All rights reserved.
Figures
References
-
- Gansevoort RT, Matsushita K, van der Velde M, et al. Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes in both general and high-risk populations. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93–104. - PMC - PubMed
-
- van der Velde M, Matsushita K, Coresh J, et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79(12):1341–1352. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
