

Economic Outcomes of First-Line Regimen Switching Among Stable Patients with HIV
- PMID: 28650246
- PMCID: PMC10397957
- DOI: 10.18553/jmcp.2017.16403
Economic Outcomes of First-Line Regimen Switching Among Stable Patients with HIV
Erratum in
-
Corrections.J Manag Care Spec Pharm. 2017 Dec;23(12):1278. doi: 10.18553/jmcp.2017.23.12.1278. J Manag Care Spec Pharm. 2017. PMID: 29172976 Free PMC article. No abstract available.
Abstract
Background: Although switching of antiretroviral therapy (ART) is a valid approach for addressing treatment failure in patients with human immunodeficiency virus (HIV), ART changes among those who are well maintained on their current regimens may lead to the development of new side effects or resistance.
Objective: To examine the effect of first-line regimen switching on subsequent health care utilization and cost among stable HIV patients.
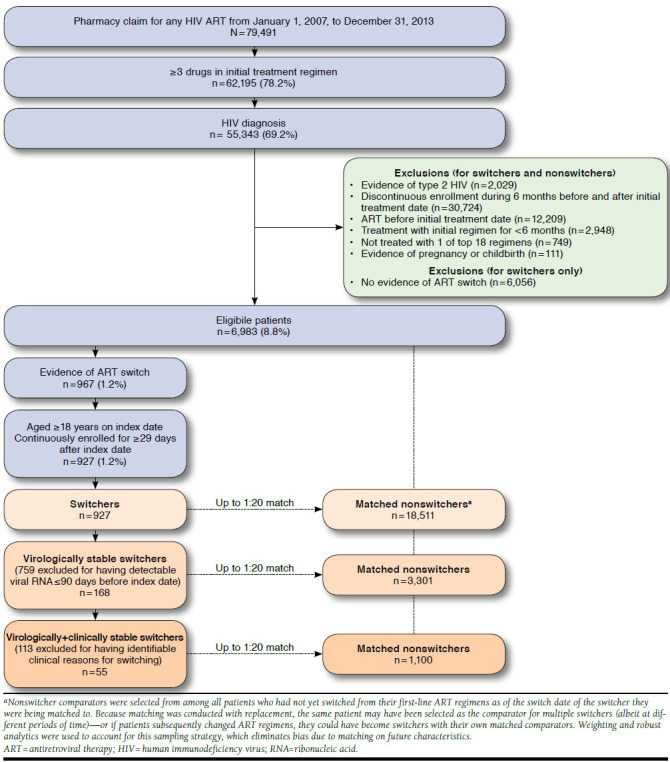
Methods: This was a retrospective claims data study of adult patients with HIV who initiated ART between 2007 and 2013 and had been treated with their initial regimens for at least 6 continuous months. Those with evidence of pregnancy or HIV-2 were excluded. Patients who underwent an ART change were assigned to a switcher cohort; a nonswitcher cohort was then generated by matching up to 20 nonswitchers for each switcher, with replacement. The index date was the date of the first ART change for switchers and was the claim date closest to the corresponding switcher's switch date for nonswitchers. Patient characteristics at baseline and post-index annualized health care utilization and costs were analyzed descriptively and with multivariable models. Analyses were performed in the full population and among patients designated as virologically stable (had undetectable viral ribonucleic acid [RNA] for 90 days pre-index) and virologically and clinically stable (had undetectable viral RNA and no apparent clinical reason for switching ART).
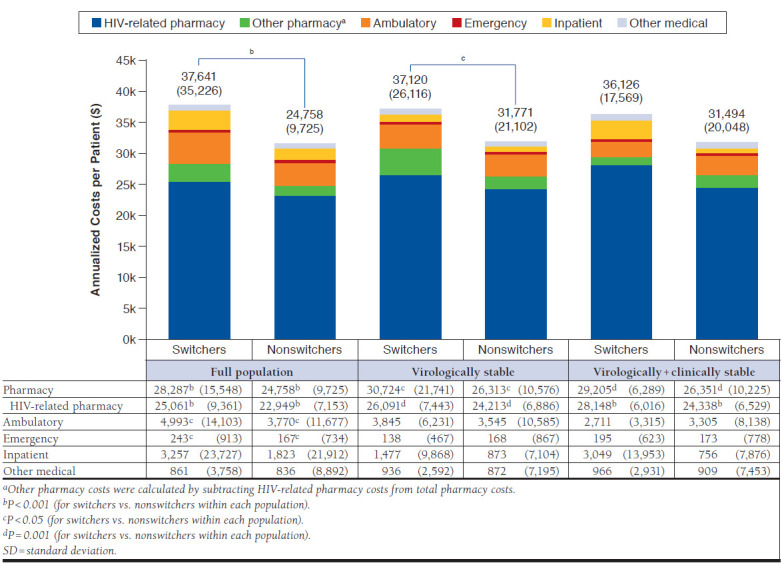
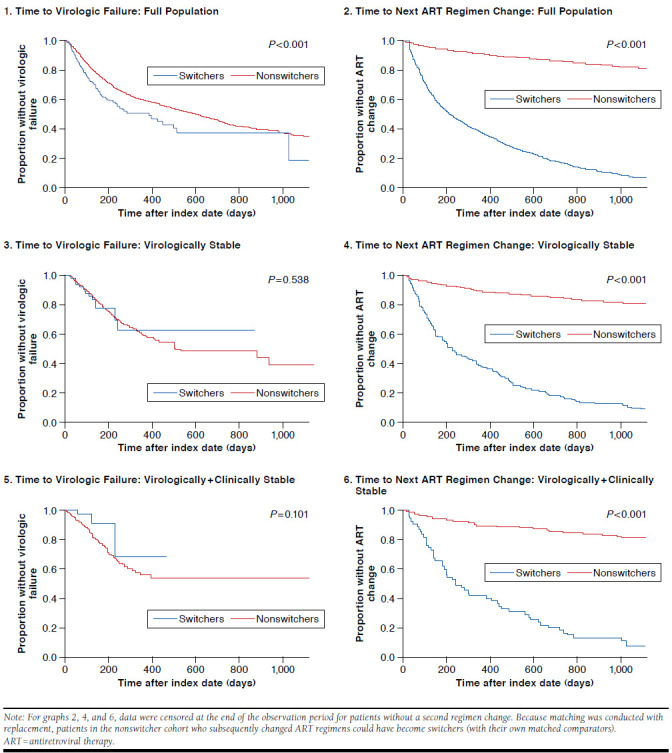
Results: The study population consisted of 6,983 individuals, which included 927 switchers (168 virologically stable; 55 virologically+clinically stable), who were matched with replacement with 18,511 nonswitcher comparators. The switcher cohort was 88.8% male (mean age 43.8 years). Mean preindex and follow-up treatment durations for switchers and nonswitchers were 1.8 years and 1.5 years, respectively; demographic characteristics, pre-index treatment duration, and follow-up duration were similar between cohorts. Significantly more nonswitchers than switchers had a first-line efavirenz-based regimen (67.2% vs. 47.8%, P < 0.001). In the virologically stable subset, follow-up annualized health care utilization for switchers versus nonswitchers, respectively, was 14.8 versus 12.3 ambulatory visits (P < 0.05), 0.8 versus 0.9 emergency department visits (P = 0.652), and 0.05 versus 0.05 inpatient hospitalizations (P = 0.915). Follow-up annualized health care costs were $37,120 for switchers versus $31,771 for nonswitchers (P < 0.05), with the difference driven largely by pharmacy costs. Multivariable-adjusted follow-up annualized health care costs were 8.9% higher among switchers versus nonswitchers (P < 0.01), and switchers also had a shorter time to subsequent ART regimen change (P < 0.001). Results were similar for the virologically+clinically stable subset.
Conclusions: In this large, real-world population, stable patients with HIV who switched from their first-line ART regimens had significantly higher health care costs than those who did not change therapies, suggesting that ART regimen changes may be costly and should be undertaken only when clinically warranted.
Disclosures: This work was funded by Bristol-Myers Squibb (BMS), which participated in the design of the study, interpretation of the data, revision of the manuscript, and the decision to submit the manuscript for publication. Rosenblatt is an employee and stock owner of BMS; Villasis-Keever was an employee of BMS at the time this study was conducted and is currently an employee of Janssen. Buikema is an employee and stock owner of Optum, and Seare, Bengston, Johnson, and Cao are employees of Optum, which was contracted by BMS to conduct the study. Optum contracts with pharmaceutical companies, such as Janssen, Merck, EMD Serano, GlaxoSmithKline, and Gilead, to conduct research in HIV. Optum is also a subsidiary of a health plan that has interest in managing the health and associated costs of patients with HIV. Study concept and design were contributed by Rosenblatt and Buikema, along with the other authors. Cao and Johnson took the lead in data collection, along with Buikema, Seare, and Bengston. Data interpretation was performed by Buikema, Seare, Bengston, and Villasis-Keever. The manuscript was written by Buikema and Bengston, along with Rosenblatt, Seare, Johnson and Villasis-Keever, and revised by Rosenblatt, Villasis-Keever, and Johnson, along with the other authors.
Conflict of interest statement
This work was funded by Bristol-Myers Squibb (BMS), which participated in the design of the study, interpretation of the data, revision of the manuscript, and the decision to submit the manuscript for publication. Rosenblatt is an employee and stock owner of BMS; Villasis-Keever was an employee of BMS at the time this study was conducted and is currently an employee of Janssen. Buikema is an employee and stock owner of Optum, and Seare, Bengston, Johnson, and Cao are employees of Optum, which was contracted by BMS to conduct the study. Optum contracts with pharmaceutical companies, such as Janssen, Merck, EMD Serano, GlaxoSmithKline, and Gilead, to conduct research in HIV. Optum is also a subsidiary of a health plan that has interest in managing the health and associated costs of patients with HIV.
Study concept and design were contributed by Rosenblatt and Buikema, along with the other authors. Cao and Johnson took the lead in data collection, along with Buikema, Seare, and Bengston. Data interpretation was performed by Buikema, Seare, Bengston, and Villasis-Keever. The manuscript was written by Buikema and Bengston, along with Rosenblatt, Seare, Johnson and Villasis-Keever, and revised by Rosenblatt, Villasis-Keever, and Johnson, along with the other authors.
Figures
Similar articles
-
Health care utilization and cost associated with switching biologics within the first year of biologic treatment initiation among patients with ankylosing spondylitis.J Manag Care Spec Pharm. 2021 Jan;27(1):27-36. doi: 10.18553/jmcp.2020.19433. Epub 2020 Oct 12. J Manag Care Spec Pharm. 2021. PMID: 33043820 Free PMC article.
-
Inhaled Corticosteroid-Containing Treatment Escalation and Outcomes for Patients with Asthma in a U.S. Health Care Organization.J Manag Care Spec Pharm. 2017 Nov;23(11):1149-1159. doi: 10.18553/jmcp.2017.23.11.1149. J Manag Care Spec Pharm. 2017. PMID: 29083972 Free PMC article.
-
Real-World Health Plan Data Analysis: Key Trends in Medication Adherence and Overall Costs in Patients with HIV.J Manag Care Spec Pharm. 2019 Jan;25(1):88-93. doi: 10.18553/jmcp.2019.25.1.088. J Manag Care Spec Pharm. 2019. PMID: 30589631 Free PMC article.
-
Estimating HIV Management and Comorbidity Costs Among Aging HIV Patients in the United States: A Systematic Review.J Manag Care Spec Pharm. 2020 Feb;26(2):104-116. doi: 10.18553/jmcp.2020.26.2.104. J Manag Care Spec Pharm. 2020. PMID: 32011956 Free PMC article.
-
Real-world clinical and economic outcomes from rapid start antiretroviral therapy in HIV: systematic review and meta-analysis.AIDS. 2025 Mar 1;39(3):241-252. doi: 10.1097/QAD.0000000000004046. Epub 2024 Oct 24. AIDS. 2025. PMID: 39453866 Free PMC article.
Cited by
-
The impact of non-medical switching among ambulatory patients: an updated systematic literature review.J Mark Access Health Policy. 2019 Oct 19;7(1):1678563. doi: 10.1080/20016689.2019.1678563. eCollection 2019. J Mark Access Health Policy. 2019. PMID: 31692904 Free PMC article.
-
Estimating the cost due to resistance against antiretroviral therapies in individuals with HIV: Perspective of the Kingdom of Saudi Arabia.IJID Reg. 2024 Apr 25;11:100371. doi: 10.1016/j.ijregi.2024.100371. eCollection 2024 Jun. IJID Reg. 2024. PMID: 38808154 Free PMC article.
-
Long-Term Benefits of Rapid Antiretroviral Therapy Initiation in Reducing Medical and Overall Health Care Costs Among Medicaid-Covered Patients with Human Immunodeficiency Virus.J Manag Care Spec Pharm. 2020 Feb;26(2):117-128. doi: 10.18553/jmcp.2019.19174. Epub 2019 Nov 20. J Manag Care Spec Pharm. 2020. PMID: 31747357 Free PMC article.
-
Economic Burden of HIV in a Commercially Insured Population in the United States.J Health Econ Outcomes Res. 2023 Jan 19;10(1):10-19. doi: 10.36469/001c.56928. eCollection 2023. J Health Econ Outcomes Res. 2023. PMID: 36721765 Free PMC article.
-
Management of the Patient With HIV/Hepatitis C Drug Interactions: A Guide for Nurses and Nurse Practitioners.J Assoc Nurses AIDS Care. 2020 Mar-Apr;31(2):241-248. doi: 10.1097/JNC.0000000000000144. J Assoc Nurses AIDS Care. 2020. PMID: 31855873 Free PMC article.
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. Available at: https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv-guid.... Accessed May 6, 2017.
-
- Stone VE, Jordan J, Tolson J, Miller R, Pilon T.. Perspectives on adherence and simplicity for HIV-infected patients on antiretroviral therapy: self-report of the relative importance of multiple attributes of highly active antiretroviral therapy (HAART) regimens in predicting adherence. J Acquir Immune Defic Syndr. 2004;36(3):808-16. - PubMed
-
- Glass TR, De Geest S, Weber R, et al. . Correlates of self-reported nonadherence to antiretroviral therapy in HIV-infected patients: the Swiss HIV Cohort Study. J Acquir Immune Defic Syndr. 2006;41(3):385-92. - PubMed
-
- Paterson DL, Swindells S, Mohr J, et al. . Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21-30. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
