

ILC2-modulated T cell-to-MDSC balance is associated with bladder cancer recurrence
- PMID: 28650339
- PMCID: PMC5531411
- DOI: 10.1172/JCI89717
ILC2-modulated T cell-to-MDSC balance is associated with bladder cancer recurrence
Abstract
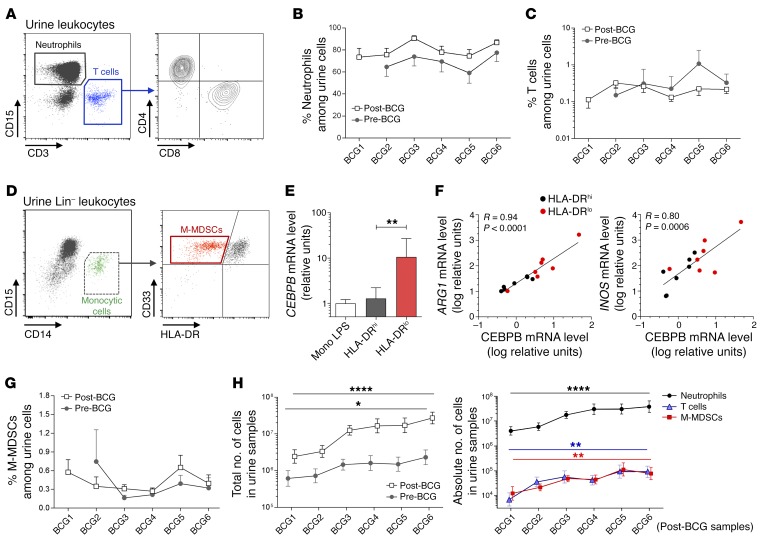
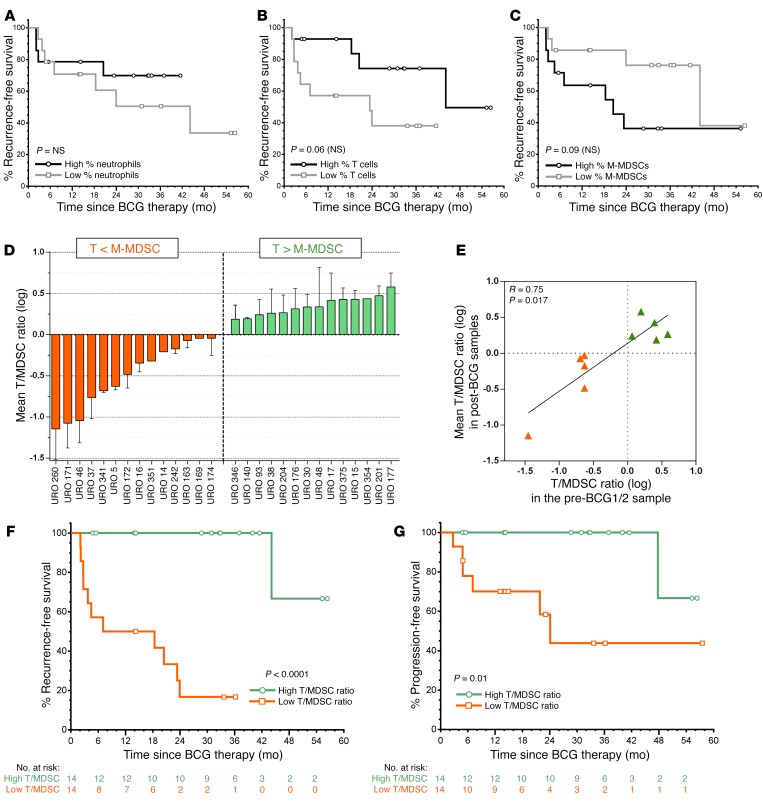
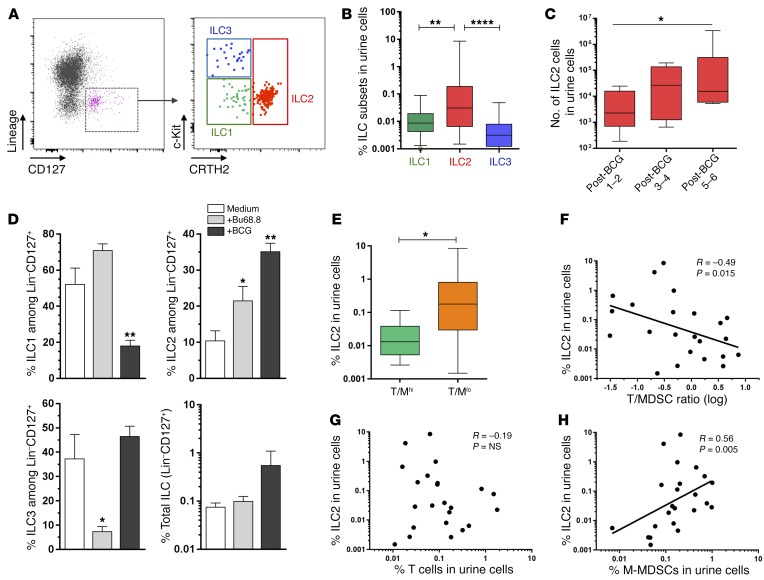
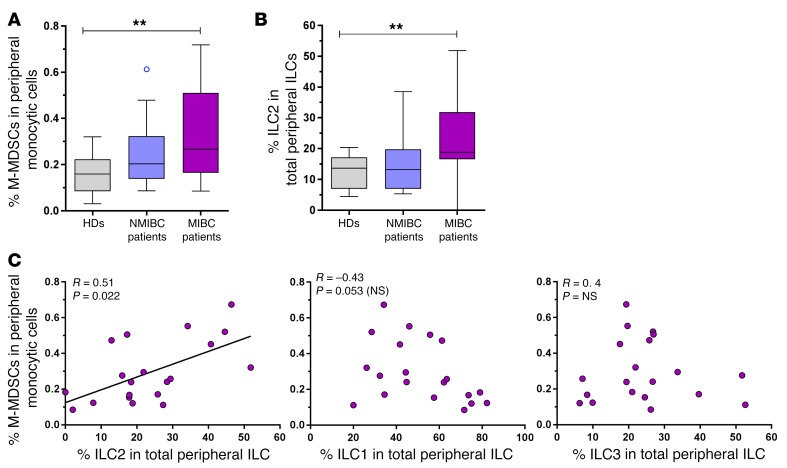
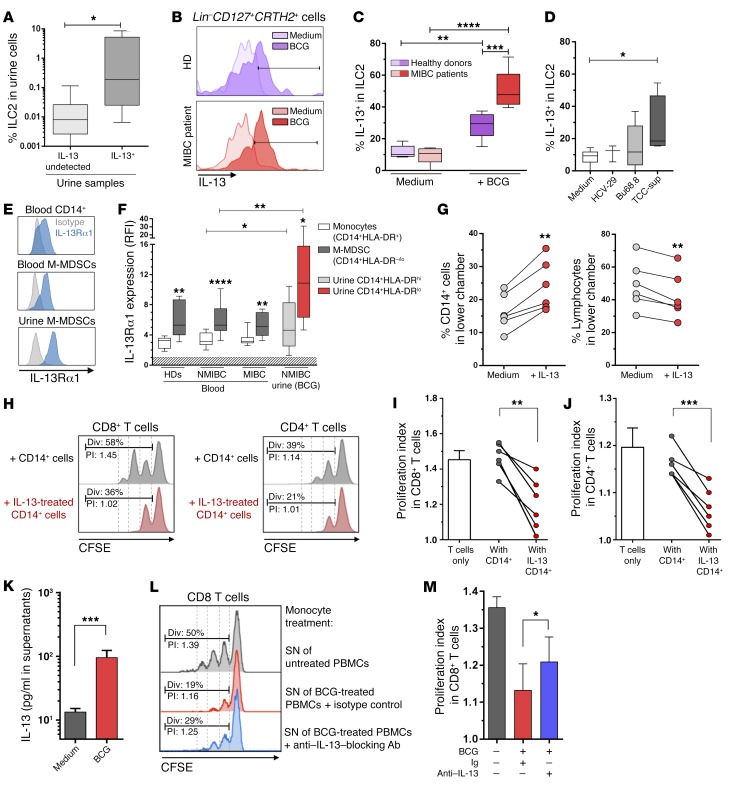
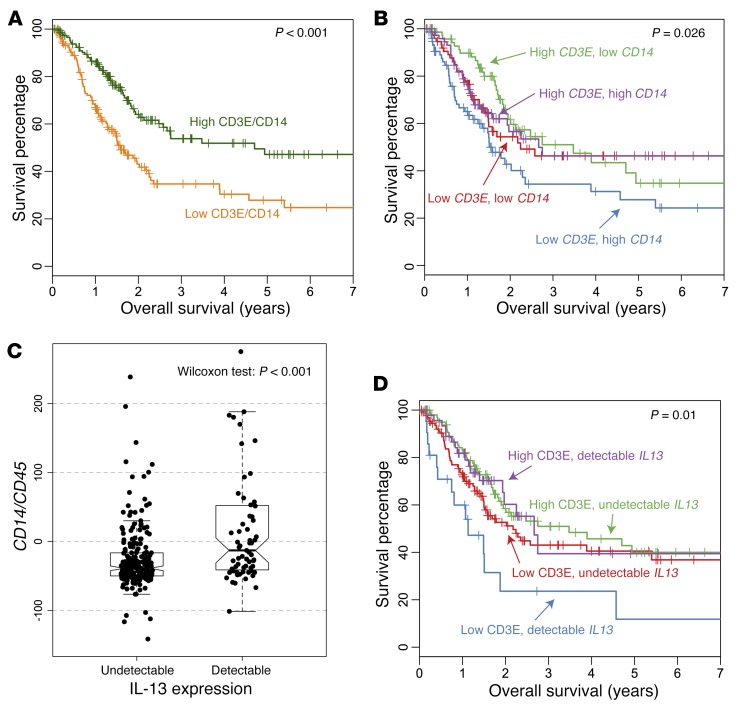
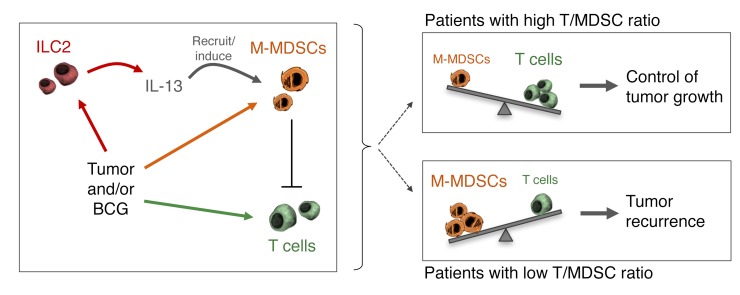
Non-muscle-invasive bladder cancer (NMIBC) is a highly recurrent tumor despite intravesical immunotherapy instillation with the bacillus Calmette-Guérin (BCG) vaccine. In a prospective longitudinal study, we took advantage of BCG instillations, which increase local immune infiltration, to characterize immune cell populations in the urine of patients with NMIBC as a surrogate for the bladder tumor microenvironment. We observed an infiltration of neutrophils, T cells, monocytic myeloid-derived suppressor cells (M-MDSCs), and group 2 innate lymphoid cells (ILC2). Notably, patients with a T cell-to-MDSC ratio of less than 1 showed dramatically lower recurrence-free survival than did patients with a ratio of greater than 1. Analysis of early and later time points indicated that this patient dichotomy existed prior to BCG treatment. ILC2 frequency was associated with detectable IL-13 in the urine and correlated with the level of recruited M-MDSCs, which highly expressed IL-13 receptor α1. In vitro, ILC2 were increased and potently expressed IL-13 in the presence of BCG or tumor cells. IL-13 induced the preferential recruitment and suppressive function of monocytes. Thus, the T cell-to-MDSC balance, associated with a skewing toward type 2 immunity, may predict bladder tumor recurrence and influence the mortality of patients with muscle-invasive cancer. Moreover, these results underline the ILC2/IL-13 axis as a targetable pathway to curtail the M-MDSC compartment and improve bladder cancer treatment.
Conflict of interest statement
Figures
References
-
- Messing EM. Why should we increase public awareness of bladder cancer, and how can we do it? Nat Clin Pract Urol. 2008;5(3):117. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
