

Incomplete viral suppression and mortality in HIV patients after antiretroviral therapy initiation
- PMID: 28650383
- PMCID: PMC5695564
- DOI: 10.1097/QAD.0000000000001573
Incomplete viral suppression and mortality in HIV patients after antiretroviral therapy initiation
Abstract
Objective: To determine whether there is a threshold of detectable HIV RNA under 1000 copies/ml after antiretroviral therapy initiation associated with 10-year all-cause mortality.
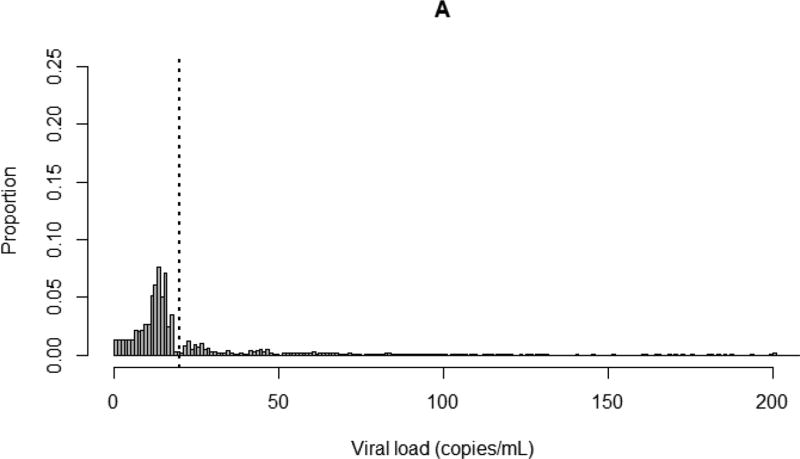
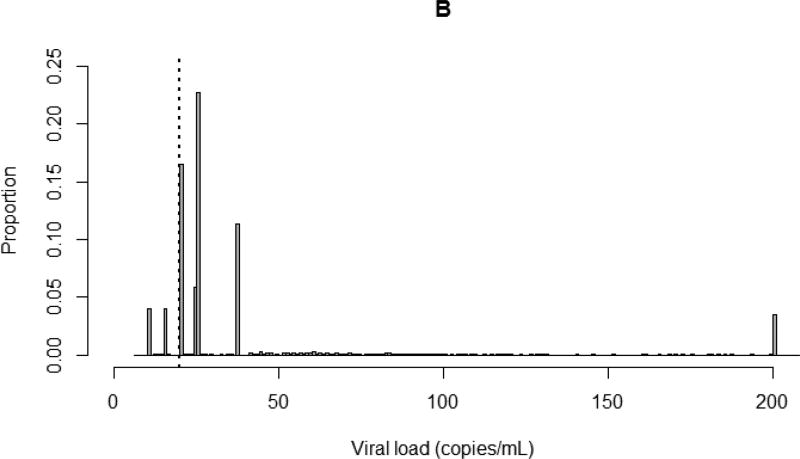
Design: This study included nearly 8000 patients from a US-based multicenter clinical cohort who started antiretroviral therapy between 1 January 1998 and 31 December 2013. Viral load was assessed 6 months after initiation of therapy. Patients were followed from 6 months after therapy initiation (between 1 July 1998 and 30 June 2014) until death, and data were administratively censored after 10 years or on 31 December 2014.
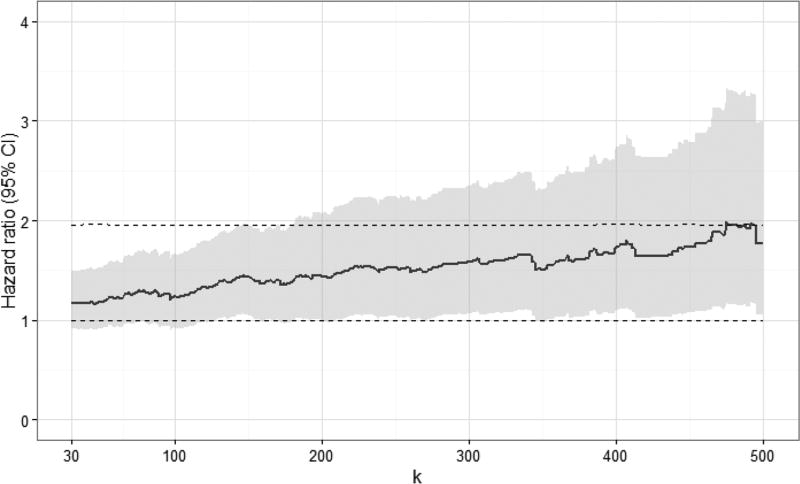
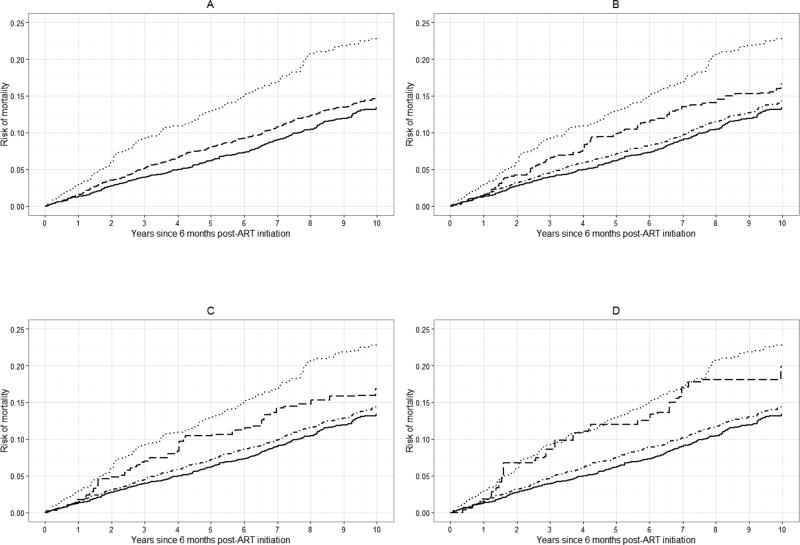
Methods: We used nonparametric multiple imputation to account for left-censored viral load measurements, Cox proportional hazards models to estimate all-cause mortality hazard ratios, Nelson-Aalen cumulative hazard estimates to construct risk curves, and inverse probability of exposure weights to standardize estimated hazard ratios and risk curves to the total study population.
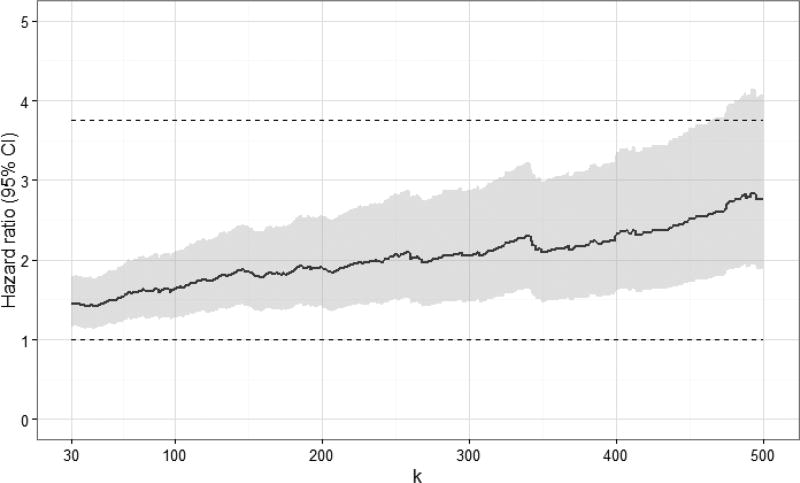
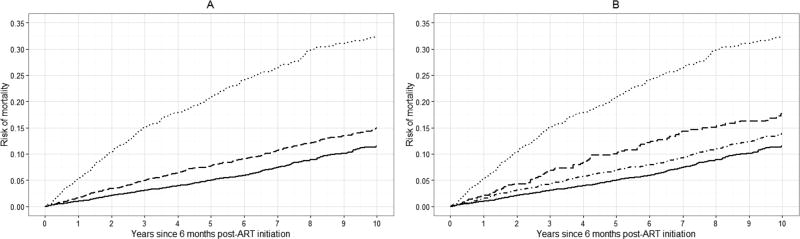
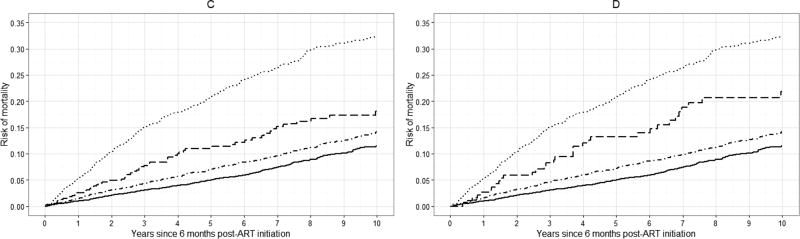
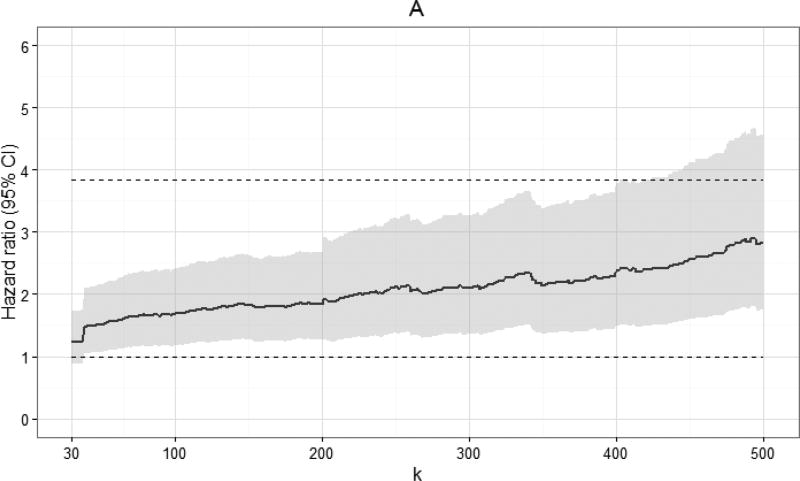
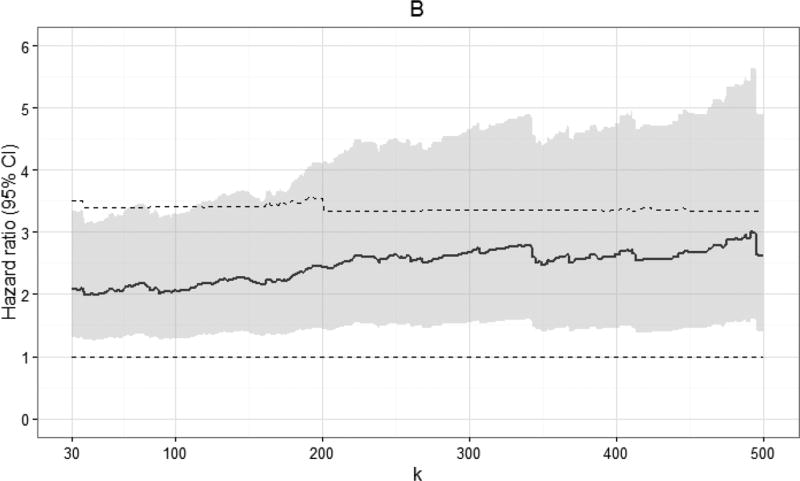
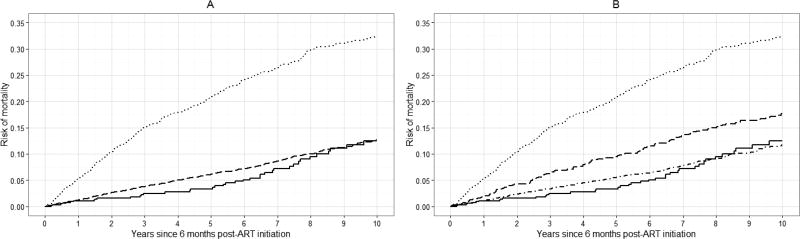
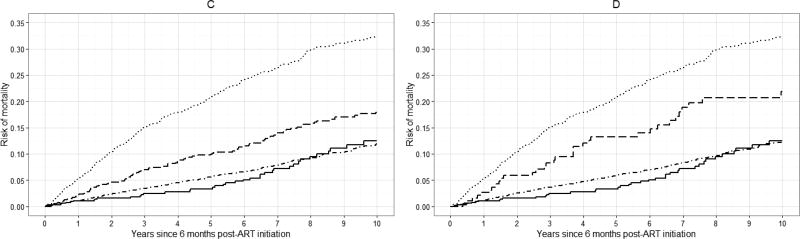
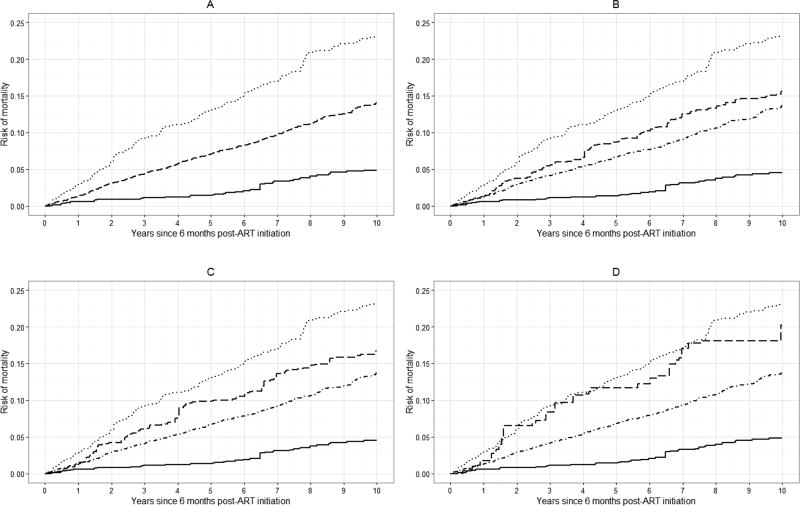
Results: Plots of standardized hazard ratio estimates and 95% confidence intervals indicated there was no demonstrable viral load threshold between 30 and 500 copies/ml associated with a marked increase in 10-year mortality. The standardized 10-year risk of mortality among patients with viral loads between 400 and 999 copies/ml 6 months after starting treatment was comparable with the risk of mortality among patients with viral loads between 1000 and 4 million copies/ml (20 vs. 23%).
Conclusion: Incomplete suppression of plasma HIV RNA 6 months after starting therapy is associated with substantial 10-year all-cause mortality risk, highlighting the importance of rapid viral load suppression after therapy initiation.
Figures
References
-
- Steigbigel RT, Cooper DA, Kumar PN, Eron JE, Schechter M, Markowitz M, et al. Raltegravir with optimized background therapy for resistant HIV-1 infection. The New England journal of medicine. 2008;359(4):339–354. - PubMed
-
- Deeks SG. Determinants of virological response to antiretroviral therapy: implications for long-term strategies. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2000;30(Suppl 2):S177–184. - PubMed
-
- Achenbach CJ, Buchanan AL, Cole SR, Hou L, Mugavero MJ, Crane HM, et al. HIV viremia and incidence of non-Hodgkin lymphoma in patients successfully treated with antiretroviral therapy. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2014;58(11):1599–1606. - PMC - PubMed
-
- Boillat-Blanco N, Darling KE, Schoni-Affolter F, Vuichard D, Rougemont M, Fulchini R, et al. Virological outcome and management of persistent low-level viraemia in HIV-1-infected patients: 11 years of the Swiss HIV Cohort Study. Antiviral therapy. 2014 - PubMed
-
- Charuratananon S, Sungkanuparph S. Rate of and predicting factors for virologic failure in HIV-infected patients with persistent low-level viremia under antiretroviral therapy. Journal of the International Association of Providers of AIDS Care. 2015;14(1):12–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
